
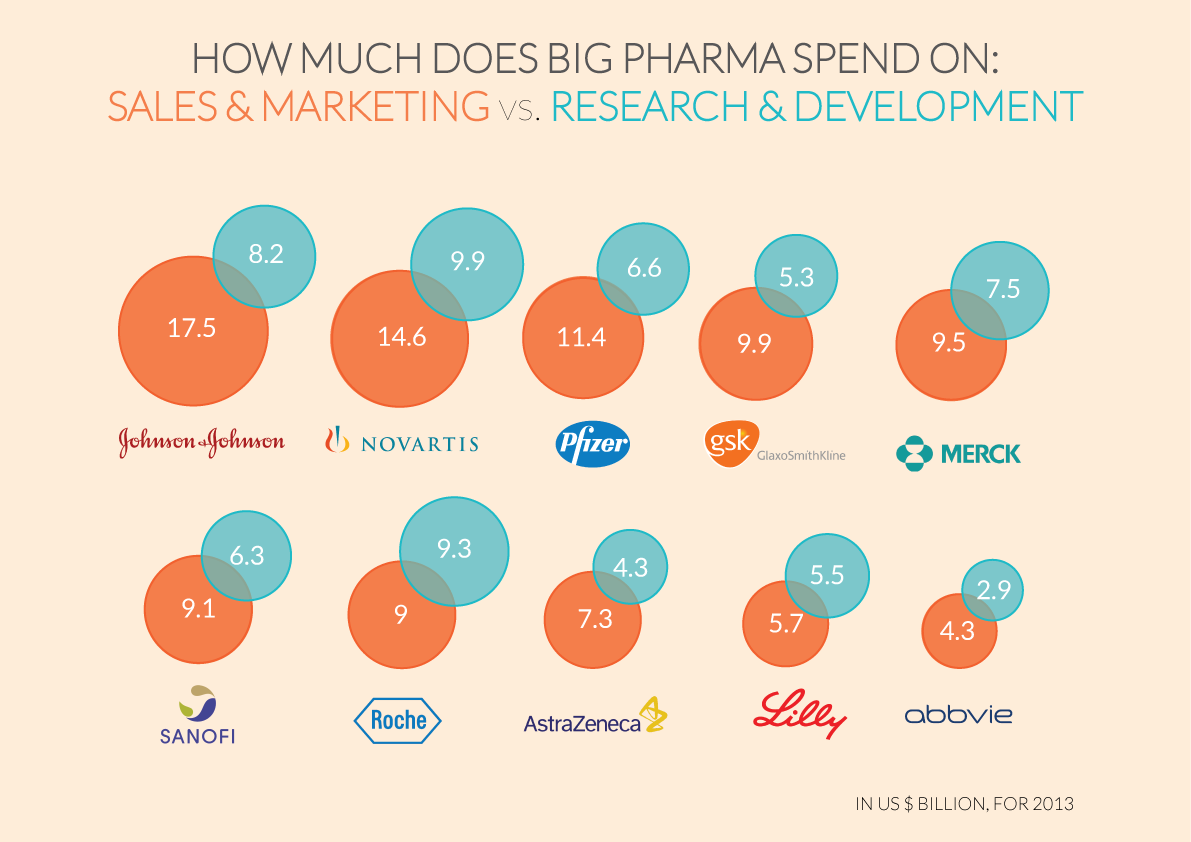
Pharmaceutical companies say that they need long patents that keep the price of their drugs high so that they can invest in research. But that’s not actually what they’re spending most of their money on. Instead, they’re spending more — sometimes twice as much — on advertising directly to doctors and consumers.
Data from the BBC, visualized by León Markovitz:
 “When do you cross the line from essential profits to profiteering?,” asked Dr Brian Druker, one of a group of physicians asking for price reductions.
“When do you cross the line from essential profits to profiteering?,” asked Dr Brian Druker, one of a group of physicians asking for price reductions.
Lisa Wade, PhD is an Associate Professor at Tulane University. She is the author of American Hookup, a book about college sexual culture; a textbook about gender; and a forthcoming introductory text: Terrible Magnificent Sociology. You can follow her on Twitter and Instagram.












{kind=link}