Inequality by (Interior) Design, a blog by sociologist Tristan Bridges, turned one-year-old last month and it is quickly becoming one of my favorites. In a recent post, Bridges featured a product that reminds us all why history is awesome: the “portable baby cage”:
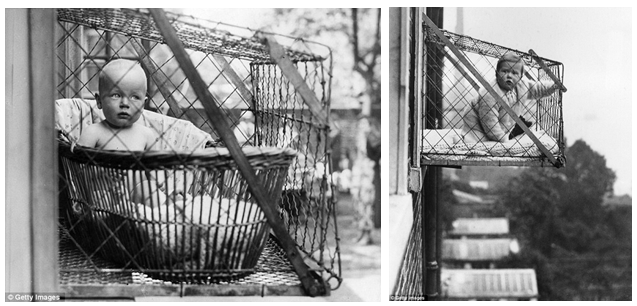

As I discussed in a previous post, with industrialization came cities and with cities came crowded, cramped living quarters. The baby cage kept infants out of harm’s way and gave the family a bit more space. As Bridges discusses, it also coincided with the idea that babies needed a lot of fresh air to be healthy. The baby cage seemed like the perfect solution.
Lisa Wade, PhD is an Associate Professor at Tulane University. She is the author of American Hookup, a book about college sexual culture; a textbook about gender; and a forthcoming introductory text: Terrible Magnificent Sociology. You can follow her on Twitter and Instagram.