This is the latest of several blogs on healthcare on ThickCulture.
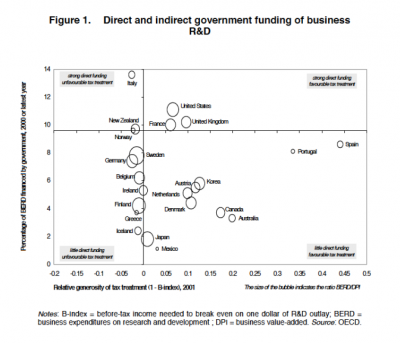
While the healthcare reform debate rages, there much emphasis on the costs. Warren Buffett has decried US health care as a “tapeworm eating our economic body”. The interesting thing is that when you look at the numbers that Buffett cite, the US is spending plenty on healthcare and has quite a few healthcare practitioners per capita. This post on the Innovation and Growth blog states the problems aren’t about the costs, but the lack of results. People are paying more, but less aggregate care is being delivered, in terms of actual better health. The blogger, Mike Mandel, also has a post posing the question of whether the US is overweight on healthcare R&D expenditures. As Ron Burgundy would say, “Compelling and rich.”
Where’s the spending going? It’s going towards the current healthcare infrastructure, insurance companies, and the research-intensive pharmaceuticals. Healthcare reform needs to address the industrial organization of the interfirm networks of the US healthcare system, so policy needs to not only have an understanding of economics, but also of organizations, strategy, and marketing. This challenges an entrenched and embedded structure of doing business, with an emphasis on business.
Real Healthcare Reform
In order to truly reform healthcare, it’s important to look at the system. Here’s a dramatically simplified representation for working Americans::
- healthcare providers -> hospitals, medical groups, & insurers -> patients
- pharmaceuticals -> insurers & pharmacies -> patients
Currently, employers and employees both pay for healthcare, with indigent care programmes and Medicare taking up the slack. Health care reform threatens how things are currently done, albeit expensively and lacking in aggregate health benefits. At some point under reform, costs will need to be addressed, which will limit total expenditures to force efficiencies out of the system. Policy aimed at squeezing efficiencies out of the healthcare system will force the players in the healthcare economic ecosystem of firms to maintain their margins to satisfy shareholders, although it should be noted that there are non-profit players in the mix. How will this impact the system?
Hospitals and medical groups will be forced to cut costs, making general medicine much less attractive as a career, due to pressure to contain wages and working conditions focusing on cost efficiencies. Already, there is evidence of this, as health providing organizations feel pressure on both ends, revenues from insurers and the high costs of labour. Under National Health in the UK, there’s increased competition amongst hospitals [1]. I see this as fostering specialization and differentiation within a government-funded system, which sheds light on how hospitals in the future may position themselves, as they compete for patients. Rural health may suffer without proper incentives in some areas, although publicly funded health may create markets for health which are current underdeveloped in others.
There will be considerable pressure to reduce pharmaceutical expenditures, which, in turn will limit the amount of pharmaceutical R&D. The pharmaceutical industry will say that this will kill future innovation, as the high prices in the US are fueling R&D expenditures, given that most of the world has price controls on pharmaceuticals. But, for all of the investment in health R&D, as noted above, it’s not as if it’s having a profound impact on aggregate health. I’m of the mind that the problem is with the traditional approach to drug development that the pharmaceutical industry engages in. A rival paradigm is one driven by medical biotechnology in the areas of using genetics in the drug development process and bioinformatics. It would be naïve to expect technology to deliver solutions in the future, i.e., that the US will innovate itself out of this healthcare jam, but what’s clear is that the current pharmaceutical model isn’t working. More is spent per revenue dollar on marketing than on R&D, so the US research-intenvive pharmaceuticals are differentiating through branding, not theraputic benefits.
The above scenario is akin to the German public/private system of health care with 82M people versus 304M in the US, so there is the issue of scalability. Nevertheless, Germany has a system with 90% opting for a public option, but here are the key points [2]::
- Both systems have providers employed in the private sector {not socialized medicine, as in the UK}
- German healthcare is financed through payroll taxes at rates that are similar to the US’ {around 15% split by employer and employee}
- German wages for physicians are half of that of US physicians at $80K, but there are wide variances in terms of hours worked and wages by specialization
- The German government sets fixed reimbursement rates and obtains price concessions from pharmaceutical companies due to its market power
- Fewer uninsured patients in Germany mean less incidence of expensive emergency care
- German hospitals don’t splurge on the latest technology, such as MRIs
- There are income barriers to enter private healthcare & older Germans cannot go back to the private system once they leave the public option
- Unemployed in Germany who have never worked still may obtain care through a social fund, the sozialamt [3]
The German system isn’t perfect and there’s questions of what the future holds, given the rapid changes in medical technologies and who will gain access to them. I don’t see the US system in its current incarnation as viable in the long term.
What about the poor insurers under health reform, I’ve blogged about in the past? If I were an insurer, I would be shifting my business model towards being what is called a “value net integrator”, a variant of systems integrator. Such an entity would focus on facilitating the data and information flows between patients, physicians, pharmacists, etc., and mining the data to help medical and policy decisions. For example, a patient’s electronic record would be in a database that could be accessed by physicians. Additionally, the “insurance company” no longer makes decisions on care, but facilitates payments from the government to the providers.
Plenty is being spent on health per capita here in the US, but I see reform in some form or another to be inevitable. Why? The private actuarial model {risk-based} of healthcare in the US is expensive, not providing enough health benefits for those covered, and too many {more and more from the middle class} are finding it hard to obtain coverage. I don’t see this as politically tenable, particularly as the economy languishes. The costs are astronomical, but the more pressing issue is that the current system is bulky and dysfunctional to say the least. Policy needs to address the entire “ecosystem” of healthcare provision, including a look at rethinking the organizational sociology, innovation, and technology when it comes to the future of healthcare in America.
Twitterversion:: Healthcare reform in the US? Are costs the focal issue or is the system fundamentally broken? #ThickCulture
Song:: Jein-“Fettes Brot”
References::
[1] Timmins, N. {2010} “Competition in NHS makes hospitals better, study says”. Financial Times. {19 February} http://www.ft.com/cms/s/0/3099e87c-1cf6-11df-aef7-00144feab49a.html
[2] Raghavan, A. {2009} “Beyond Hysterics: The Health Care Model That Works”. Forbes. {1 September} http://www.forbes.com/forbes/2009/0921/health-obama-germany-health-care-model-that-works.html
[3] Green, D. Irvine, B., & Cackett, B. {2005} “Health Care in Germany”. Civitas. http://www.civitas.org.uk/pubs/bb3Germany.php