One morning as I was sitting toward the back of a 5th grade classroom, Carmen, a Black girl—extremely devoted to academics—was completing her math assignment. She raised her hand to ask the teacher a question. Ms. Josephine, her white teacher, asked Carmen to wait. Carmen kept her hand raised—she did not want the teacher to forget about her. Ms. Josephine raised her eyebrows and rolled her eyes at Carmen. Carmen, embarrassed by this visible impoliteness in front of the entire class, resisted by rolling her own eyes. Ms. Josephine saw this and said loudly, “Barbie right here, she needs more cheese with her wine…” Everyone laughed. Later that day when Carmen wanted to use the bathroom, Ms. Josephine said, “You just come pretty every day and you want to go to the bathroom to chat.” Everyone laughed at Carmen again. Her eyes filled with tears; Carmen put her head down on her desk before the tears could roll down her cheeks.
As a wave of bills and legislations to suppress conversations around racial oppression and privilege sweeps the US, and white parents debate the right time to teach their kids about race, I bemoan the futility of these conversations. The reality is that regular racial harassment, cruelty, and indifference is a common experience for Black and brown students inside schools. And this should be the urgent conversation on race and public schools.
The hostility that racially marginalized students, particularly Black and immigrant girls of color, experience inside their classrooms and schools every day is not unleashed by police and School Resource Officers alone.
From 2017 to 2020 I followed a cohort of economically marginalized Black, Latinx, Asian, and recent immigrant students, in a large metropolitan public-school district in western US, documenting their journey from 4th to 6th grade. Inside the classrooms and corridors, over and over again, I witnessed teachers harass Black girls and immigrant girls of color.
Just as Black girls like Carmen were harassed and reduced to their sexuality, robbed of their innocence and girlhood, immigrant girls of color were harassed drawing on caricatures of the immigrant. Like Ms. Luft, a white 4th grade teacher, who mocked a supposed “Asian Accent,” laughing and joking with her colleagues at lunch, as some 4th graders who had returned early from lunch pointed and laughed at their classmate Kevin—whose parents were Chinese immigrants.
Even Black and immigrant girls, like Carmen and Kevin, who excelled in the classroom, as per white middle-class standards, were not immune to racist harassment.
Moreover, I watched how teachers repeatedly refused to acknowledge Black and immigrant girls’ intellect even when they excelled as per white middle-class standards. Like when Eliza’s white 5th grade teacher discounted the fact that she had remained at the top of her class (in math and English) through 4th and 5th grade by arguing that Eliza just “works a lot” unlike a white girl who simply “has this knack for reading.” Her teacher argued that “she [Eliza] is at top is kind of like fake.” And, when Gloria, who had recently immigrated from Michoacán, wanted to participate in class discussion her teacher either plainly told her that she was not legible by her classmates (most of whom, I noted, understood her very well and were themselves bilingual), or when Gloria spoke in class her teacher simply narrowed her eyes and shook her head side to side to indicate confusion at what Gloria said and then ignored her answer.
Sometimes immigrant girls of color were used as the vehicle to harass Black girls. Like when a teacher working with a group of “lower-ability” English learners told a Black girl in the group, “Maria [a recent immigrant] has an excuse. Her family, they don’t speak English. What makes you sit here,” implying that the Black girl must lack intelligence or is lazy.
Sometimes teachers used the example of Black girls at the top of the class to deride Black girls who did not meet academic standards urging that if “those just like them” can succeed then others must just be “dumb.” They did the same thing to immigrant girls of color. For example, when Mariana continued to perform well academically despite her father’s deportation, she was used as an example of grit. Mariana was not allowed to mourn her father’s deportation and the resultant trauma in her family. Teachers told other immigrant girls of color that they simply weren’t good because Mariana’s situation was “proof” that anyone “just like them” can do well.
Of course, teachers of color can also engage in racial harassment. I found that Black girls were harassed even by teachers who seemingly had the most radical race politics. I want to note, however, that the teachers and administrators in the schools I studied, as well as the larger district, were overwhelmingly white just like much of the education profession. And harassment most often came from white teachers.
Teacher pay is also decidedly exploitative and they often work in hazardous conditions with minimal resources. But this truth coexists with widespread teacher racism. What I found is not surprising either; it is reflective of the regular coverage of teachers racially harassing students across the nation.
My research warns us that academic achievement is a fundamentally incomplete, and even dangerous, way to understand how marginalized students experience school. Schooling, different from education, has in fact historically served as a way to stifle Black freedom and assimilate colonized people and Third-World immigrants into the state.
The focus of attention on the achievement gap reflects an incomplete understanding of schooling. Simply having marginalized peoples at the top of the classroom (or positions of power) is insufficient. While integration and diversity projects in education center, and benefit, whiteness and white people, we also need more than anti-racist trainings for educators.
It is time to follow the lead of generations of Black and Third World scholars and activists, and transform how we conceptualize schools—from an idealized site of potential liberation to its reality as a site where violence may be experienced. Because what we need is a future where marginalized communities have the right to self-determine their educational freedom.
Ranita Ray (@ranitaray1) is Associate Professor of Sociology and Maxine Baca-Zinn Endowed Chair at the University of New Mexico. She is the author of The Making of a Teenage Service Class: Poverty and Mobility in an American City—the 2018 C. Wright Mills Award Winner. Supported by NAEd/Spencer Foundation, she is currently writing a book on the everyday gendered-racial violence of schooling and the proliferation of race discourse in contemporary United States.
Jeremy’s parents divorced when he was three. For the first two years after the divorce, Jeremy saw his father every Tuesday and every other weekend, but this decreased dramatically when his father remarried and moved to Nevada, where his new wife’s family lived. At that point, the custody arrangement switched to one week during the holidays and one month over the summer. His mother, Sherry, didn’t remarry because she didn’t want to introduce more men into Jeremy’s life. Her mother had done that when she divorced Sherry’s father, and she’d vowed never to repeat that behavior with any child of her own.
Sherry had struggled with depression much of her life, and suddenly being a single mother with a small child and little spousal support didn’t help matters. She couldn’t afford therapy to ease her depression, so she worked hard, read parenting books, and paid attention to the advice offered on shows like Dr. Phil, Dr. Laura, and Oprah. Plus, Jeremy was a quiet kid who kept his head down, did his studies, and didn’t give her any trouble, even as a teen. And because he was a good student, he was able to get a full scholarship to a decent liberal arts college in the Midwest.
But their relationship started to change when he went to college. When he first arrived, Jeremy called or texted his mother once a week to let her know that he was doing okay and making friends, since he knew that she was a worrier. However, that very quickly tapered off to once a month, as he became involved in his schoolwork and new social life. He eventually stopped responding to his mother’s calls and found himself feeling burdened by her complaining and personalizing his distance. The more that she complained about his unavailability, the less he wanted to talk to her.
His father had been reaching out to him again after years of little contact, and he found himself excited about the possibility of reestablishing their relationship. After a difficult breakup with a girl in his dorm, he started seeing a young psychologist, referred to him by the counseling center. As part of their work together, the psychologist told him that his mother suffered from narcissistic personality disorder. He also recommended that Jeremy take a break from his relationship with her and focus on himself.“Anger is active: it can cause us to feel like we’re pushing back, rather than feeling victimized by the outcomes of our lives.”
By the time that Sherry contacted me, Jeremy hadn’t spoken or written to her in almost two years. I emailed Jeremy to see if he’d be open to talking with me about his mother.
He responded right away, and we spent a session talking about his mother on the phone.
I liked talking to him. He seemed thoughtful, insightful, interested in his own psychology. While he was critical of his mother, it was clear that he also cared about her and didn’t want her to suffer. I also discovered that his therapist was a bigger obstacle than were the criticisms of his mother.
– – – –
Therapists can do a lot of damage. We can encourage a divorce from a spouse who’s more amenable to change than we realize, harming the lives of the client and her children. We can encourage someone to stay in a marriage that creates ongoing depression for him or his kids. We can support a parent who cuts an adult child out of a will, without confronting how much he has contributed to the child’s negative behavior. We can support an adult child’s decision to end a relationship with a parent without being sensitive to how that decision may affect the client, his children, and the parent who’s being cut off.
Perhaps a more important problem than blind spots resulting from our inexperience, unexamined prejudices, or limited orientations, is that therapists’ perspectives often uncritically reflect the biases, vogues, and fads of the culture in which we live. If you were a therapist in the 1950s and a woman showed up at your office claiming she was unfulfilled in her role as a mother and housewife, most likely your goal would not be to propel her into a career or into more meaningful activities outside of the house. Instead, you would investigate what prevented her from being happy with what made other women, ostensibly, so contented. Her boredom or lack of fulfillment with domesticity, an ideal at odds with the culture at the time, would be viewed as a neurosis to be treated with medication and psychoanalysis.
This example is just one in a long history where psychotherapy and the medical community labeled perfectly natural discontents with or reactions to prevailing social arrangements as “diseases” that must be treated, rather than issues that must be addressed. Here’s another: In 1850, Dr. Samuel Cartwright reported in The New Orleans Medical and Surgical Journal the discovery of a new disease, which he called drapetomania. Drapetomania was a condition that caused sulkiness, dissatisfaction, and a desire to avoid service. It was used to describe slaves who sought to run away from their servitude: drapetes, the ancient Greek word for “runaway slave,” and mania for “excessive energy or activity.”
These examples demonstrate how the failure of therapists to challenge the social, economic, racial, and gender norms of their time led them to translate adaptive behaviors, or at least understandable discontents, into illnesses. Today’s therapists continue this tradition by failing to critically examine new cultural and societal trends that often serve to lessen wellbeing and increase family conflict and division.
One of the more profound ways that our culture has changed in the past century is in its embrace of the individual as separate from the family and the community at large. Today’s culture of therapy both reflects and contributes to our nation’s ever-growing embrace of individualism. While prior to the 1960s, the aims of psychotherapy were generally to encourage people to conform to the institutional dictates of the time, today’s therapists and self-help authors want to help their clients become more resistant to the forces of guilt, shame, and worry about others that stand in the way of their developing their talents and pursuing their dreams. To that end, family members have increasingly come to be viewed as facilitators of (or obstacles to) a fully realized life, rather than necessary and forgivable features in an expectably imperfect existence. While the family was once where individuals located themselves in a chronological or social order, it now comprises the institution from which they must be liberated.
With the exception of parenting small children, encouraging individuals to feel some sense of obligation or care for family members is not typically on most therapists’ agendas. As a result, an adult child’s psychotherapy can sometimes increase family conflict and distance. Unless a client requests help in having a better relationship with the parent, sibling, grandparent, or in-laws, most therapists worry that too much emphasis on the needs or feelings of the person outside of the room will be antithetical to helping their client focus on their own needs—which is, after all, the point of much therapy today.
As therapists, we hold up the ideal parent or family experience as a way to shine a light on what an adult’s life might have been if she’d had better parenting. This serves the purpose of helping our client to not blame herself for self-limiting and self-hating voices, and to allow her distance from parents and others whose contact tends to amplify that voice, rather than diminish it. It also allows a creative space to imagine what she might feel or accomplish without the critical voices, that may have brought her into therapy in the first place, whatever the origin.
Helping adult children see what they didn’t get and what they should’ve ideally gotten from parents is one of the biggest tools in a therapist’s tool chest, and one that I go to on a daily basis. An analysis of a client’s childhood is useful because parents and siblings can powerfully shape identity, self-esteem, feelings of trust or safety in the world, and later, one’s ability to parent. Psychotherapists can be efficacious teachers about the relationship between the adult child’s functioning as an adult and the family’s contribution to those inadequacies, deficits, or conflicts.
But there’s a downside to that. In so doing, therapists tempt adult children to feel contempt or even hatred for their parents. They may encourage their anger because anger is powerful: it can carry anger away from the self. In blaming others we’re relieved of the self-blame, the shame, and the guilt we feel about our defects and our failures. Anger is active: it can cause us to feel like we’re pushing back, rather than feeling victimized by the outcomes of our lives. But in the same way that hating the sin and not the sinner still involves hate, supporting anger or contempt for a parent doesn’t necessarily free the adult child from that from which they hope to be freed.
Family Therapy with Jeremy and His Mom
After speaking with me on the phone, Jeremy agreed to do a few sessions with his mother and me. Sherry was right that Jeremy was a kind, quiet person. But a kind nature can sometimes be a burden; it may overly weigh you down with feelings of guilt and responsibility for those you love. In my experience, sometimes the nicest kids have to become the most aggressive to reassure themselves they’re not responsible for another’s wellbeing.
I had counseled Sherry before our first family therapy session, attempting to prepare her for what was to come. I’d advised: Listen in a non-defensive way to whatever Jeremy has to say. Try to find the kernel of truth in his assertions, however hurtful they may be. Even if his words are at odds with your memory and self-reflections, try to hear it as his perspective and not a matter of right or wrong.
In my solo session with him, I recommended that he directly tell his mother what bothered him. Jeremy didn’t hold back. He didn’t dilute his perceptions or try to shield her from being hurt. It seemed as though he was waiting for this moment to get all of this off his chest, which I supported because I wanted him to get as much on the table as soon as possible.
“You chose to stay in bed with your depression when I was young instead of deciding to get up and fix yourself,” he began. “And as a result, I’ve had a much harder time knowing how to do basic things in life or prioritize my own needs in relationships. My therapist said that I was parentified by you and that you were emotionally incestuous with me growing up. That’s why I haven’t wanted to talk to you. I need to work on myself.”
I had wanted him to be direct. But I also knew that I would need to translate his words—products of his own therapy—which, undeciphered, sound like the worst kind of character assaults: “emotional incest,” “parentified,” “narcissistic personality disorder.” These, the flora and fauna of the Diagnostic and Statistical Manual, can sound pretty humiliating to those on the receiving end.
Softening the bite of psychiatric diagnoses is especially important, since they are now an active part of mainstream culture. We call someone “borderline” or “a total narcissist” when we used to say “jerks” or “assholes.” We might still call them that, but putting it in the context of a diagnosis sounds so much more authoritative.
While diagnosing is perhaps an unavoidable part of living in a society obsessed with personal growth and development, labels have consequences and can affect the behavior of those doing the labeling as well as those being labeled. In the same way that a diagnosis of cancer or Alzheimer’s may cause family members to increase—or, in some cases, decrease—contact, so too, can a psychiatric diagnosis affect people’s attitudes toward those to whom they’re related.
In this poignant example, Jeremy wasn’t exactly wrong in his assessment about what he didn’t get from his mother or how it may have shaped his life. There’s ample evidence that being raised by a depressed parent (most of the research is on mothers) can have a negative effect on the child. And he very likely did grow up feeling more responsible for his mother’s wellbeing than he might have preferred or than might have been useful to him—though there’s other research that shows that the strengths learned from that role can also be a positive. But he was blaming his mother for behaviors she would’ve done differently if she’d known how, or if she’d had the psychological or economic resources when she was raising him.
Do People Choose to be Bad Parents?
There is often less free will when it comes to parenting than most realize. Parents are as much under the throes of their genetic dictates, partner provocations, childhood traumas, financial threats, and community deprivations as are the children being parented. Sherry’s deficits in parenting stemmed not only from her own parents’ deficits, but also from her financial struggles, her genetic and environmental vulnerability to depression, and her lack of having another parent with whom to share responsibility raising her son.
Our current construction of causality in the family—where therapeutic discourses lead people to believe that choice is the organizing and guiding principle of life—often create more conflict in families than it solves. From Jeremy’s perspective, his depressed mother should have or could have just pulled herself up by her bootstraps, gotten out of bed, and marched herself into a therapist’s office.
Studies show that most adult children explain their estrangements based on the personal traits in the parent that caused their behavior, rather than contextual, economic, or cultural mechanisms. However resonant that causal framework is with American ideals, it fails to describe how depression works, how decision-making works, or even how choice works.
For the child under a therapist’s guidance to later look back and say that the parent should’ve known better or behaved differently—that they now deserve the distance, if not the contempt, they receive—is wrong. It suggests that the parent was handed a map for a geography that wasn’t yet charted when they were raising their children and given resources that were beyond their reach.
This is not to in any way minimize the enormous amount of damage—sometimes permanent—that problematic parenting can cause. Children raised by those who were emotionally or physically abusive, or neglectful due to mental illness or alcohol or drug addiction, know firsthand the pain that can be caused by parents. That pain can radiate out into all aspects of his life. Telling an adult child “I did the best that I could” may be small consolation to someone who suffered for many years as a result of the parent’s behavior. And it provides scarce motivation for the adult child to engage in a process of reconciliation. This is why I encourage parents to do due diligence on their children’s complaints and work hard to repair whatever harm was done.
Misdiagnosing the Parent
Jeremy’s therapist wasn’t wrong that his mother needed more love, caretaking, and tenderness than he could reasonably be expected to provide. Nor that the incompatibility of their temperaments may have created genuine suffering in him. But in my experience, many therapists misdiagnose a mother’s maternal depression as narcissism. Depressed mothers can be more needy, anxious, and sometimes disparaging. Therapists might interpret this depression as narcissism or some other personality disorder.“Carl Jung wrote that nothing affects children more than the unlived lives of their parents. I sometimes discover, underneath the contempt a client feels for the parent she has rejected, a deep reservoir of sadness for that parent and a longing for them to be happy.”
Did Jeremy’s mother have narcissistic personality disorder, as he and his therapist believed? She did not. More important, that diagnosis foreclosed the possibility that they could together build a bridge of understanding where Jeremy—without guilt or regret—could accept the limitations of what he could or should provide his mother and his mother could accept—without bitterness or complaints to her son—that his care and attention would never be enough to make up for the difficult hand that life had dealt her before and after becoming a parent.
Jeremy’s mother did deserve a better life. It just wasn’t necessarily her son who could provide it. And Jeremy deserved a better life, too. It just wasn’t necessarily his mother’s fault that he lacked it. Giving the mother a psychiatric diagnosis, especially one as outsized and definitive as narcissistic personality disorder, greatly oversimplifies her life and struggles; it devalues her years of love and dedication, however flawed; and it weakens the fabric of connection that could otherwise have existed. She deserved a different narrative, one that was deeper and more compassionate, that saw her less as a freewheeling agent, more as someone responding to what life offered her from what she had to offer in return.
Carl Jung wrote that nothing affects children more than the unlived lives of their parents. I sometimes discover, underneath the contempt a client feels for the parent she has rejected, a deep reservoir of sadness for that parent and a longing for them to be happy. The parent’s sorrows, frustrations, feelings of inadequacy become so burdensome that the child doesn’t know any other way to shed that weight other than to write her off. As author Andrew Solomon wrote in Far from the Tree, “There is no contradiction between loving someone and feeling burdened by that person; indeed, love tends to magnify the burden.”
What some adult children find oppressive about their parent may not be the parent’s personality disorder, as is so commonly highlighted in therapy offices and on forums, but the weight of their own feelings of empathy.
– – – –
For the adult child, the decision to estrange the parent, however painful, is nonetheless tied to a narrative of liberation from oppressive forces and the pursuit of happiness. There is no equivalent upside for the parent. It’s all downside: failing at life’s most important task; being denied the valued reflection of oneself as a parent; feeling shame before one’s peers and family; losing not only the adult child, but often a relationship to cherished grandchildren. And for those parents who are all too aware of their parental failures, they also lose the opportunity to do for grandchildren what they couldn’t for their own children.
Jeremy’s mother had a hard time with the first few sessions. Her chronic depression made her less able to hear her son’s complaints as complaints and not as an attack on her fundamental worth. But, as often happens, her ability to just listen, reflect, and find the kernel of truth helped him to see that she was stronger than he had given her credit for. And it also helped when she was able to tell him that while she did miss him and would like to be in more contact, she didn’t need him in the way that he thought she did—to give her life purpose—and that it wasn’t selfish of him to be more focused on his own life and less focused on hers. They talked about a way to be in contact going forward. It would be less than she wanted, but so much more than she had before.
Reconciliation therapy between parents and adult children is similar to couples therapy where one member is willing to call it quits. For those open to considering a deep examination of the foundational problems in the relationship, a marriage can sometimes be saved and, in many cases, made better than ever. The same can be said for estranged parents and their adult children.
Joshua Coleman, PhD, is a psychologist in private practice and senior fellow with the Council on Contemporary Families. Coeditor with historian Stephanie Coontz on a compendium of research on the contemporary family, he is also a cofounder of Standing Together, a center for advancing awareness of family estrangement. Follow them on Twitter @drjcoleman
In 2021 the movement to oppose abortion rights experienced a banner year. By the midpoint of 2021, according to the Guttmacher Institute, state legislatures or municipalities enacted more abortion restrictions than in any other year since Roe v. Wade. In September, the United States Supreme Court declined to block Texas Senate Bill 8, a law that effectively bans abortions in Texas after six weeks and institutes a bounty system that enables private citizens to sue anyone assisting a patient seek or obtain an abortion. Beginning in December 2021, the Supreme Court will hear oral arguments for Dobbs v. Jackson Women’s Health Organization to consider the constitutionality of a Mississippi law that bans abortion after fifteen weeks of pregnancy. Widely viewed as a referendum on Roe v. Wade, the Court’s decision may drastically alter women’s rights to reproductive healthcare.
Amidst these legal rollbacks, a larger, quieter faction of the antiabortion movement works “to overturn Roe v Wade in hearts, not just the courts.”
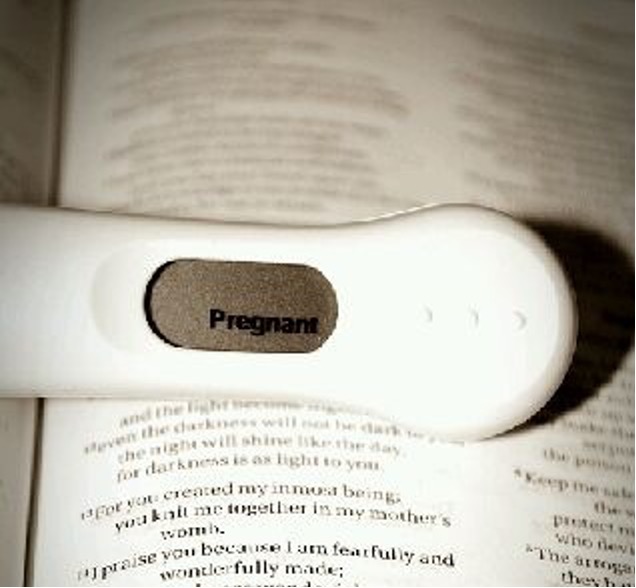
Pregnancy centers—also termed crisis pregnancy centers (CPCs) or pregnancy resource centers (PRCs)—are non-profit, faith-based organizations that provide, in their words “alternatives to abortion.” While centers desire, in the words of one network organization, “to make abortion unwanted today and unthinkable for future generations,” they stay largely out of the legal fray. Instead, they position themselves as ministries that, like in Texas, are ready to help women when clinics that provide abortions empty. It is this concept of ‘ministry,’ that I write about in an article* recently published in Gender & Society.
What are Pregnancy Centers?
Pregnancy centers offer free resources like urine pregnancy tests, options counseling, limited obstetric ultrasounds, and material services (e.g., diapers, infant clothing, and car seats). They can provide confirmation of pregnancy that helps clients enroll in Medicaid and many refer to a network of social service providers and offer parenting classes. Some offer STI testing, medically unfounded “abortion-pill reversal” services, and unsubstantiated “post-abortion counseling.” Centers are increasingly professionalizing and medicalizing (estimates hold that approximately 70 percent now offer ultrasounds under the licensure of a physician). However, most are led, staffed, and supported by evangelical Christian women and only offer services that align with their religious worldview. Thus, they do not provide nor refer for contraceptive or abortion care, instead advocating for abstinence outside of marriage and ‘natural family planning’ within marriage. More troubling still is evidence provided by a variety of studies that pregnancy centers disseminate medical misinformation about abortion and contraception, and craft websites that obfuscate their services and mission. Though pregnancy centers are not full-spectrum healthcare providers, some receive state and federal funding.
These centers comprise a distinct movement within the broader antiabortion movement that is uniquely evangelical and gendered. While the patriarchal ideology that infuses conservative evangelical Christianity tends to keep women out of positions of power in churches and other evangelical groups, pregnancy centers are led by women who use this gendered ideology to articulate and defend approaches to abortion opposition that focus on women’s presumed needs. This approach is popular. Pregnancy centers, draw more volunteers who put in more hours than any other part of the moment. Indeed, with somewhere between 2,500 and nearly 2,800 centers across the United States they outnumber, by a wide margin, facilities that offer abortion. Despite this vast reach, most women cannot distinguish between a pregnancy center and an abortion provider and new research conservatively estimates that approximately 13 percent of pregnant people visit a center during their pregnancy. My research sheds light on these centers, by focusing on the concept of ministry and how it shapes centers’ tactics and performance of care.
Ministry Not Manipulation
Pregnancy centers identify as “faith-based” and, most centers, like the two that I studied over the course of three years, are seeped in evangelical Christianity. Centers’ founders, leaders, and supporters—most of whom are evangelical Christians—describe their work as a ‘ministry.’ And, as is typical of centers in the U.S., they affiliate with large, evangelical network associations (like Care Net,Heartbeat International, or NIFLA) that define the goals and strategies of affiliates. A key part of their ministry? Evangelism.
For instance, Care Net holds that the primary mission of the pregnancy center is to share the gospel of salvation with clients, while Heartbeat International promotes centers as an “unparalleled opportunity for relational evangelism” giving “young women in the throes of perhaps her most trying time…a thoroughly gospel-saturated response, pairing a Christ-centered offer of hope with a real-world commitment to walk alongside another.”
Given these endorsements, imagine my surprise when I did not see Bibles handed out, tracts dispersed, or staff sharing personal testimony with clients. “Ministry not manipulation” was an oft repeated phrase in centers and at trainings that staff unpacked in in-depth interviews. They painted a portrait of relational evangelism that is uniquely gendered, a process I refer to as feminizing evangelism. In learning to practice feminized evangelism, staff—who avowedly hate abortion—come to empathize with women considering abortion on the basis of shared, gendered experiences. They articulate a unique ministry that they hope is more effective than other approaches to evangelism. However, staff consciously work to realign their deeply felt religious beliefs with practices that require them to put the Bibles away and to avoid conversion conversations.
Feminized evangelism gains more widespread support and client trust. In removing overt ‘God talk’ from appointments, centers produce a narrative of care that is grounded in social welfare and wrapped in the language of ‘empowerment’ and ‘trauma-informed care.’ While staff emphasize that they don’t hide their faith, most clients in my study did not realize the pregnancy center they visited was “faith-based” prior to their first appointment. Over the course of my fieldwork, both organizations gained secular and nonsecular supporters across the political spectrum, and solicited referrals from various secular organizations (including, unsuccessfully, a local Planned Parenthood). Pregnancy centers are not held to the same regulatory and credentialing requirements as healthcare facilities, Further, their religious orientation restricts the range of services provided and shapes how they deliver them, information that most women want to know. When that worldview is not transparent, clients cannot give informed consent to services.
Supporting people with resources that enable them to build families if, when, how, and with whom they want should be a priority for our country. Excluding contraceptive and abortion care from reproductive support does the opposite. Pregnancy centers believe that providing limited economic resources and empathetic counsel enables meaningful choices but the ability to make unconstrained reproductive choices depends equally on access to a full range of healthcare services, including abortion and contraception.
The Supreme Court’s decision on Dobbs, not expected until 2022, may restructure the landscape of abortion care. Pregnancy centers are ready to fill the void and patients. If they do, patients with few resources—those who are low income, underinsured, live in rural areas or conservative states, or women of color—will bear the consequences of religiously-based healthcare restrictions.
*This is freely available to read, download, and share through Open Access.
Kendra Hutchens is a research associate at Circle A Productions and a lecturer at the University of Colorado Boulder. Her academic research explores crisis pregnancy centers and Americans’ abortion attitudes. In the public sector, her research focuses on deinstitutionalization for individuals with intellectual and developmental disabilities.
Once they are ready to have a baby, many heterosexual couples expect that having sex to get pregnant will be the fun and easy part. They are often surprised to discover that sex for the explicit purpose of conceiving bears little resemblance to how they think that sexual intimacy should be. What, exactly, is going on?
I conducted interviews with 52 mostly advantaged White women in the United States married to men who attempted to get pregnant via sexual intercourse. Most of this sample is drawn from a study of individuals and couples who failed to become pregnant via sexual intercourse and went on to pursue fertility treatments, with a subsample who successfully conceived via timed intercourse.
I found that rather than sex being driven by desire, sex for the purpose of pregnancy is driven by cisgender women’s ovulation cycle, with couples attempting to optimize the timing of sex in order to maximize their chances of successfully conceiving. Having sex on a schedule makes it feel more like a chore that needs to be completed than an intimate moment. More than that, it is a chore that mostly falls on women. Sex for pregnancy ends up being a “third shift,” that is, extra work in addition to women’s paid work and unpaid household work (Hochschild 1997).
There are three different types of work involved in sex for the purpose of pregnancy. The first is body work (Gimlin 2007). Women need to monitor their ovulation cycle, with many taking their temperature, using ovulation predictor kits, checking their cervix, and entering data into phone apps or spreadsheets. The second is cognitive labor (Daminger 2019). Once they determine when they are supposed to have sex, they must coordinate their schedules with their husbands to make sure that they are both available to have sex at the right time. The third is emotion work (Hochschild 1979). Because in many heterosexual couples there is the expectation that men should initiate sex, many women also perform desire to make their husbands amenable to having sex at the best time for conception.
To illustrate the experience, here are the words of one participant explaining what it was like to have timed intercourse:
…when I finally started ovulating again, it was very like, ‘Okay. Now here we go.’ Now everything’s chugging along and sex was like, ‘Come here Tiger, put a baby in me.’ And four, five, six, seven months go by and it’s no longer sexy, ‘Come here and put a baby in me.’ Now, it’s like, ‘I have egg white cervical mucus. I know you’re tired but we’re doing it tonight.’ That’s just not sexy.
This participant did not want to “force” her husband to be part of the “non-sexiness,” however. She tracked her ovulation schedule on her own, tried not to talk about when the right time of the month for sex was, and when it was the right time, she attempted to seduce her husband, making it seem like they were having sex because she was aroused rather than because there was a greater chance that she would conceive that night. She said that all of this body work, cognitive labor, and emotion work was “exhausting” and “stressful.”
In fact, many study participants reported that having timed intercourse was hard on their marriages, some so much so that they accelerated their entry into fertility treatments in a medical setting so that they could stop having sex on a schedule. This study shows that sex for the purpose of pregnancy rather than being ‘normal’ is actually experienced as a deviation from heterosexual couple’s normal nonprocreative sex lives. The contemporary cultural ideal is that sexual intimacy is supposed to be driven by spontaneity and desire, not by reproduction. In fact, in my previous research, I found that advantaged women were so concerned about their romantic lives being determined by their reproductive timelines, that they decided to freeze their eggs (Brown and Patrick 2018). Ultimately, sex resulting in pregnancy is very different from—and often understood to be preferrable to—sex for the purpose of pregnancy.
On a practical level these findings suggest that just as medical professionals consider the sexually acceptability of different contraceptive methods, they might also consider how different methods of promoting pregnancy affect couple’s sex lives. On a more theoretical level these findings illustrate that when thinking about household chores, it’s important to remember that any activity can become a chore—and more than that, a gendered chore—depending on the context.
References
Brown, Eliza, and Mary Patrick. 2018. “Time, Anticipation, and the Life Course: Egg Freezing as Temporarily Disentangling Romance and Reproduction.” American Sociological Review 83: 5: 959-982.
Daminger, Allison. 2019. “The Cognitive Dimension of Household Labor.” American Sociological Review 84: 4: 609–633.
Gimlin, Debra. 2007. “What is ‘Body Work’? A Review of the Literature.” Sociology Compass1: 1: 353–370.
Hochschild, Arlie Russell. 1979. “Emotion Work, Feeling Rules, and Social Structure.” American Journal of Sociology 85: 3: 551–575.
Hochschild, Arlie Russell. 1997. The Time Bind: When Work Becomes Home and Home Becomes Work. New York, NY: Metropolitan Books.
Suggested Citation
Brown, Eliza. 2022. “Less Like Magic, More Like a Chore: How Sex for the Purpose of Pregnancy Becomes a Third Shift for Women in Heterosexual Couples” Sociological Forum. DOI: 10.1111/socf.12803
Author Bio
Eliza Brown, PhD, is a postdoctoral fellow in sociology at University of California-Berkeley. Her research has been published in American Sociological Review, Social Science & Medicine, and Sociological Forum, and covered in media outlets such as The New York Times Magazine and The Atlantic. She is currently writing a book about twins related to fertility treatments. You can find them on Twitter @ElizaBrown_
At the first Mardi Gras ball I attended in Baton Rouge, Louisiana, my host Ernest appeared in elaborate drag at the end of the event, debuting as the queen of the ball. His parents and siblings from rural Louisiana crowded at two tables to celebrate his entrance. They wore pins signifying that they were the parents of the queen, they wore crowns from their own experiences as royalty at Mardi Gras events. They stood and celebrated the entrance of Ernest onto the raised stage in a convention hall filled with over one thousand guests.
When I started my research on lesbian, gay, bisexual, transgender, and queer (LGBTQ) involvement in Mardi Gras in the Gulf South, I had no idea that family would be a central part of my research. Mardi Gras or Carnival season is celebrated throughout the Gulf South from mid-January to the start of Lent. Private organizations called krewes or social aid and pleasure clubs organize the festival by hosting parades and private balls. There is a long history of LGBTQ krewes throughout the Gulf South that dates back to the early 1960s. In my book Queer Carnival, I analyze how these festival events are central to how LGBTQ people make a place for themselves in the Southern city. I argue that involvement in Carnival is fundamentally about cultural citizenship, cultivating a sense of belonging in one’s own city.
But just as important is the way that these events are an opportunity for LGBTQ adult children to connect with their parents and other family members. Over two-thirds of the LGBTQ adults I spoke to in this research had family members who attended their festival event. Discussions about family involvement in krewe events were the most emotional parts of my interviews, as interviewees often cried when they talked about their parents attending. Largely, these family members were not “PFLAG parents” (i.e., Parents, Families, and Friends of Lesbians and Gays) or people who identify as strong allies, yet they showed up to publicly support their LGBTQ children.
Parents were involved in many aspects of festival events. Several lesbian festival Queens and Kings received money from family to help with costs, particularly for their royalty expenses the year they were the queen or king of the ball. The mother of one white lesbian paid for her royalty gown and train with funds that had originally been put aside for her wedding. I was conducting this project as same-sex marriage was being legalized statewide, and so many interviewees described family support as equivalent to the money and attention they might have lavished on a wedding.
These connections can even be reconciliatory, repairing damage done to parent-child relationships in volatile reactions to coming out. The most dramatic story came from James, a younger white gay krewe member in Baton Rouge. James had an ambivalent relationship with his mother. When he came out at age eighteen, she kicked him out of the house. A tumultuous decade later, James was costuming for the first time and invited his mother to attend the ball. James bought her a ball gown, had her come early so that the krewe could do her hair and makeup, and made sure her favorite cocktail was on hand. “She had a day, it was nice,” James told me. He did what I have termed “comfort work” to make attendance at the ball comfortable for her. James reported that after the ball she was immediately enthusiastic and told him she wanted to help him decorate his table and making the food for the event next year. James’s mother attended his mostly-LGBTQ house party during a neighborhood festival parade the next weekend. His mother hung out in his kitchen during the party, making gumbo, and insisted later that James’s friends refer to her as “Mama Zee.”
Mardi Gras is just unexpected space that allows parents to show up for their LGBTQ children. This project pushed me to think more broadly about the ways that parents may support their LGBTQ adult children and youth. I think more about the myriad ways that parents show up (or don’t) for their children.
Amy L. Stone (they/them) is Professor of Sociology and Anthropology at Trinity University and author of Queer Carnival, Gay Rights at the Ballot Box and Cornyation: San Antonio’s Outrageous Fiesta Tradition, along with being co-editor of Out of the Closet, Into the Archives: Researching Sexual Histories. They study lesbian, gay, bisexual, and transgender (LGBT) politics, urban life, and health. They co-lead two project, Family Housing & Me/Familia Casa e Yo and the community-based research project, Strengthening Colors of Pride, in San Antonio. You can follow them on Twitter @AmyLStone1
Op-ed by Barbara J. Risman, Senior Scholar, Council on Contemporary Families, Distinguished Professor of Sociology, University of Illinois at Chicago
In my city of Chicago, our Mayor Lori Lightfoot, is a woman. Dr. Allison Arwady is Chicago’s commissioner for Public Health. Our county commissioner is another woman, Toni Preckwinckle and so is our District Attorney Kim Foxx. Three of the four are women of color. Women run this city, if not the world.
Joyful beautiful young woman in superhero costume posing on sunset background.
When I was young you never saw visible women beyond the president of the Temple Sisterhood, or the PTA. Little girls had few role models for living a life beyond domesticity. Much has changed in American society. I now live in a city where finding a man in charge in public life isn’t easy. Oh yes, the President of the predominantly female teacher’s union. And he’s at the top because, of course, white men ride glass escalators to the top. While much has changed, some things remain the same.
Still, young girls today have all sorts of role models. You can be not only a mother or teacher or nurse, but also a successful politician, a doctor, or a lawyer. You can even be a Vice-President, or run for President, and maybe be the first woman to break that glass ceiling.
This is all good. And yet, male privilege refuses to give up the ship. Many of those female teachers and nurses, politicians, doctors and lawyers are suffering disproportionately in the pandemic because mothers retain the primary responsibility for childrearing in our country. And now childrearing has to be done with erratic schooling and day care centers that close for weeks at a time. No one is to blame for a worldwide pandemic, but the disproportionate disruption suffered by mothers, instead of to all parents, can definitely be blamed on a certain group of people, heterosexual men. What is wrong with fathers? It is more than half a century past the first surf that crashed introducing the second wave of feminism and still many men in heterosexual relationships are often deadbeat fathers and husbands even when they stay married to the mother of their children. Mothers need day care and schools in session face to face to carry on with their lives, and function in their own jobs. But why isn’t that true for fathers as well? I’ve been studying gender inequality for four decades and I still don’t understand why otherwise good men are not good enough to be egalitarian partners. And why do otherwise smart and even high earning women put up with such men? Why don’t the rest of us shame them? Do you know a hetero man who passively lets his equally busy wife handle most of the household labor, including childcare and now online schooling during a pandemic? How about treating him with as much disapproval as you show to someone refusing a vaccine. He may not risk killing other people like anti-vaxxers but he sure is disrespecting his own wife and providing a great role model of patriarchal privilege to his kids, both boys and girls. Isn’t that bad enough to deserve public humiliation?
While little girls are watching all those role models, they notice the women in their lives shouldering a double shift, earning a living and doing most of the work it takes to keep a family going. Little boys are noticing that once you get married, you have someone to take care of you and your kids. Great lessons in normalizing male privilege.
As women make progress in the world outside our homes, we all quickly realize that having women in charge doesn’t necessarily make the world a safe or healthy place. No one could argue that my city, Chicago, with women running the show, from the city and county chief executives, to the justice and health systems is any kind of feminist utopia. Of course, they did inherit systems created and screwed up by men. Do women lead differently, better, then men? It’s too early to tell. How would we measure that? Some research suggests they do, as women organizational leaders become change agents, at least improving women’s status. But what if women as a group, are not any better at their jobs then men are?
Isn’t that the point? Women have as much right to run the world as men do, whether or not they do it any better. But my money is on the women leaders in my city doing a better job than the men before them. Hard to do worse. Just as important, men have as much responsibility to care for their children as do women, whether or not they parent any differently. Children, and their mothers, deserve no less.
Barbara J. Risman, Senior Scholar, Council on Contemporary Families, Distinguished Professor of Sociology, University of Illinois at Chicago. You can follow them on Twitter @bjrisman
Why did you write this book? I wrote it because I strongly believe there is no closure after the loss of someone you love. From my 40 plus years of working with ambiguous loss around the world, I learned about the myth of closure, people who love relatively well despite living with a loss that has no clarity or official verification. So, I wanted to write a book about this misuse of the term closure for some time.
I started this book several years ago, but then my husband required care and I set the manuscript aside. After he died in 2020 (of a stroke, not COVID), and the shutdown from COVID continued, I picked up the manuscript again and finished the book. What surprised me is that it’s now a very different book from the one I began writing several years ago. It is personal, it’s about topics I never addressed before (personal ambiguous loss, racism, climate change). Importantly, it’s not a therapy book, but I hope it’s therapeutic– for whomever reads it, ordinary readers as well as professionals. After nearly two years of pandemic, political upheaval, and racial injustice and disparities, people are highly distressed, if not traumatized, right now, and need help. This book does not pathologize or offer a medical model, but rather is more social psychological and a way of thinking that is stress based and meant to help us cope with this unprecedented time of trouble.
(1) Why is closure a myth? Isn’t that what people want after loss?
Closure is a perfectly good word in real estate or when a road is closed after a flood, but it’s a hurtful word in human relationships. Using it after loss makes people think there will be an end to the pain, but in fact, we live with grief and don’t get over it. Of course, it is lessened over time, but we keep the lost person in our heart and mind. Closure is not necessary nor achievable. Often, it is a misnomer in that what people really yearned for which is clarity, certainty, or justice about one’s loss. People want the certainty of loss, proof, justice not closure.
(2) What is ambiguous loss and how does it differ from losses with a clear finality such as a validated death?
Ambiguous loss is an unclear loss that has no resolution. There are two kinds: Physical and psychological. Examples of physical ambiguous loss are soldiers missing-in-action, children kidnapped, migrants who disappear, etc. More common examples of physical ambiguous loss result from divorce and adoption. The lost person is gone, but not for sure. There is no proof of death.
Psychological ambiguous loss results when the person is present, but their mind or memory is disappearing. Examples are Alzheimer’s disease the and the over 80 other illnesses or conditions that lead to dementia. The person is there but not there.
(3) What ambiguous losses have we experienced during the pandemic and how do they affect us? Physically, we have lost the ability to touch those we love, to be with them in the hospital or care facility when they are ill or dying. Until recently, young people have been separated from friends and classmates, while rituals of life, such as weddings and funerals have been limited to just a few people or virtual events. Psychologically, we have lost trust in the world as a fair and safe place, we have lost our feelings of safety when out among the public, etc. The book goes into this more.
(4) if the pandemic (or another crisis) forces us to adapt and change, is that a good thing? Well, the pandemic is not a good thing, but learning to adapt and change is a good outcome to a bad situation. It increases our resilience and our tolerance for ambiguity so we can better cope with other troubles that may come down the road. (5) And why might some people refuse to change and adapt to crises, (wear a mask, get vaccinated) while others adapt and change? Some people remain absolute thinkers when the problem is ambiguous. The virus is invisible, the scientists understandably can’t talk in absolutes, the losses remain unclear– so if one is an absolute thinker, you pick an absolute answer to the trouble. In this case that means, “It’s a hoax, I don’t need to wear a mask, nor get vaccinated. It’s all about MY freedom, not my community.” Such absolute thinking is also evident when people say, “You’re either for me or against me;” “People are either dead or alive; there is no ambiguity,” so they declare a missing person dead prematurely and they don’t’ see the in between, the nuance.
The Council on Contemporary Families (CCF) seeks applicants for the CCF Scholars Early Career Program. The CCF Scholars Early Career Program offers a unique professional development and mentorship opportunity to early-career scholars conducting research on American families. The program offers selected scholars mentorship from senior scholars who will provide them guidance and support to promote their research to journalists and the media.
Through participation in the CCF Scholars Early Career Program, early career scholars will attend a virtual summer-long program consisting of four professional development seminars and three one-on-one meetings with their mentors, including peer networking activities and training in public scholarship with other scholars. In the Fall, they will attend a special one-day event at Ohio State University to present their research to the board of CCF, meet their mentors in person, and receive further training, mentoring, and networking opportunities with board members and each other.
Each CCF Scholar will receive an allocation of $750 towards travel and complimentary CCF membership for two years. Scholars will also work to produce a research brief, fact sheet, or blog post about their research that CCF will publish and disseminate to the media. These experiences will enable scholars to gain valuable skills to promote their research on American families to media outlets and allow them to interact not only with their selected mentors but also with other scholars and professionals.
Eligibility
Ph.D. completed by May 2022.
Early career professional (i.e., doctoral degree granted within seven years or less, or current postdoc or assistant professor). Scholars from diverse disciplines are encouraged to apply. Current CCF members include demographers, economists, family therapists, historians, political scientists, psychologists, social workers, sociologists, communication scholars, as well as other family social scientists and practitioners.
Research program is broadly consistent with the mission of CCF to enhance the national understanding of how and why contemporary American families are changing, what needs and challenges they face, and how these needs can best be met.
Has a draft of an unpublished manuscript that addresses an important problem, process, or issue in the science or practice of American families. Data should be analyzed, and manuscript should be in progress with plans to submit to a peer-reviewed journal.
To Apply
You must submit the following materials to the Council on Contemporary Families no later than April 8, 2022, by 11:59 p.m. PST:
A one-page cover letter detailing why you are interested in the program, your research interests and experience, and career goals.
An abstract of the manuscript in progress, including methods, results, and key findings, that will be the focus on the training in the program.
A curriculum vitae (CV).
A letter of recommendation from a mid-career or senior scholar supporting your application for the position. Recommenders may submit their letters of recommendation at the following link: https://forms.gle/CFFxH76MH1pnJCb69
Single people are often pressured to find a new partner in our “couple culture,” where the idea that some people might want to be single seems, to many, unthinkable. The benefits to (and limits of) monogamous relationships have long been critiqued by feminist scholars asserting that heteronormative coupling lacks mutual respect, desire, intimacy, and pleasure. Embedded in these critiques of human relationships is the notion that people want to be in relationships with one another. Perhaps, but for some people, after a second, third, or fourth divorce, they decide to single lives. How many major breakups would it take for you to decide that human relationships simply just aren’t for you?
In my research, I wanted to know why some people own what are usually called “sex dolls” (e.g., life-sized sex toys resembling a human person) and better understand how doll owners compare their sex practice to human sexual relationships. I conducted digital ethnographic fieldwork among the online love and sex doll subculture—a group of people who gather online to share with one another about the highs and lows of synthetic companionship. For 14 months spanning 2020 and 2021, I posted on message boards, hung out in chatrooms, followed dolls, doll owners, and doll companies on social media, and conducted interviews with 41 people. I met people living with synthetic companions living in North America, Europe, and Australia. My goal was to interview a diverse sample of doll community members, so I purposefully sampled men, women, and queer doll owners, the partners of doll owners, and people who work in the adult industry.
A common thread among doll owners is dissatisfaction with human relationships. Few doll owners are young and inexperienced. Rather, most doll owners are 40 years or older, have been in one or multiple long-term relationships, and after experiencing a particularly bad breakup, have chosen to move on from human relationships. It’s also true that the typical doll owner is a heterosexual man. These commonalities result in a culture that centers men’s experiences and desires. Some men expressly blame feminism and liberalism for their relationship woes and suggest that modern relationship expectations are unrealistic. Other men within the community actively resist this framing and do not blame women for their predicament. They simply prefer to be single. Nonetheless, what connects doll owners is desire for intimacy and sexual pleasure, just not with a human.
By no means do heterosexual men have a monopoly on intimate hardship. Women, queer, and trans people can also become tired of trying to find a relationship that meets their wants and needs. Although most dolls cater to heterosexual men, doll companies pride themselves on customizability and variety. As such, single people spanning a diverse spectrum of gender and sexual identities are beginning to find synthetic companionship attractive. For marginalized doll owners, the default masculine discourse of the doll community is off-putting, especially so for women, many of whom hope that the stigma associated with sex dolls will erode as more people chose synthetic companionship. One woman who is a content moderator for a prominent doll forum named Helen compared the stigma of synthetic companionship to the rights of sexual minorities. She said, “I think as more people buy dolls and more dolls are out there in the public eye, it will become more accepted. It’s a generational thing. Compare it to Stonewall, you know? Who would, who would imagine that after Stonewall, 30 years later, they would legalize gay marriage nationwide? I mean, that would be, that would have been unthinkable.”
Importantly, synthetic companionship is not restricted to single people. Dispersed among the community I also met people using dolls in ways that challenge heteronormative monogamy. Some couples use dolls to fulfill extramarital desires, while others leverage the customizable aspect of dolls to have sex in transgressive ways. Because genital configurations can be swapped with ease, queer doll owners use their dolls in ways that challenge normative understandings of gendered bodies and desires. For example, Sean, who is in a polyamorous marriage with his AFAB non-binary wife, purchased a doll to have a girlfriend. Additionally, since Sean also enjoys being anally penetrated during sex, he also bought a penis attachment that he can put onto his doll Gracie to change her sexual functionality.
As we advance further into the 21st century it is likely that technology will continue to play an increasing role in sexuality and intimate relationships. Research on dating apps has exploded in recent years as more and more people use online dating to find partners. And while some attention has been paid to sex dolls, most of this research has been theoretical rather than empirical. Perhaps this is because few acknowledge that people are already living synthetic lives. But they are, and understanding how social forces shape the decision to forgo human relationships will be crucial in understanding this controversial sex practice.
Kenneth R. Hanson is a Doctoral Candidate in the University of Oregon Department of Sociology. He researches how and why people use technology to fulfill sexual and emotional desires, cultural narratives about sexual transgressions, and gendered sex practices. You can find him on Twitter @Ken_R_Hanson
Funding acknowledgements:
Lawrence Carter Graduate Student Research Award, University of Oregon Department of Sociology
Research Award for Data Collection and Presentation, University of Oregon Department of Sociology
For those wanting to end a pregnancy, the cost of in-clinic abortion care can be a significant barrier. The average cost of medication abortion (abortion with pills) in a clinic is $551. The majority of people pay for their abortion out of pocket. Abortion funds help cover some of the in-clinic abortion costs for some people, but they are not able to assist everyone in need of financial help. Many people who struggle to pay for their abortion delay or forgo paying bills such as rent, food, or utilities. The lack of affordable access to abortion care in the United States is linked to ongoing personal financial distress, debt, and poor credit.
Restrictive abortion laws in the U.S. add further economic burdens to people who would like to obtain an abortion in a clinic. At the federal level, the Hyde Amendment bans insurance plans that use federal funds, such as Medicaid, from paying for abortion care. Restrictions at the state level, such as mandatory waiting periods and multiple visit requirements, add costly appointments to the in-clinic experience. Restrictions aimed at abortion facilities, such as requiring that they be fitted out like mini-hospitals, have closed many clinics. These closures have placed additional financial burdens on people seeking in-clinic abortion care by necessitating out-of-pocket costs such as childcare, lodging, transportation, and lost wages.
As abortion has become increasingly restricted, researchers have found evidence that some people in the U.S. forgo the clinic altogether. Instead, they manage their abortion on their own, outside of the formal healthcare setting. While some people have attempted abortion self-management with methods such as herbs, teas, homeopathic remedies, or self-harm, the growth of information-sharing on the internet has brought expanded access to the abortion medications mifepristone and misoprostol.
In 2018, Aid Access became the first service to provide self-managed medication abortion in the U.S. via an online telemedicine service.
This brief reports on a recent study of 80 U.S.-based people who self-managed their abortion using medications obtained from Aid Access. The in-depth interviews, conducted anonymously, sought to understand the role that socioeconomic factors play in an individual’s decision to self-manage an abortion using online telemedicine.
Key Findings
The main reason why participants sought abortion care via online telemedicine was the unaffordable cost of in-clinic abortion.
Restrictive state abortion policies, on top of personal financial hardship, made it impossible for participants to access abortion care in a clinic.
For participants with children, their family’s economic wellbeing motivated the decision both to seek an abortion and to do so via online telemedicine.
Medication abortion provided via online telemedicine offered an affordable alternative to the high costs of in-clinic abortion care. However, for some, accessing pills at no cost or a reduced cost was necessary because the suggested donation of $90 still posed a financial burden. See representative quotes below.
The high costs of in-clinic abortion care, made more difficult by restrictive abortion policies – along with balancing the needs of existing children – motivated people to seek medication abortion via online telemedicine
Note: Quotes have been edited for brevity.
Policy Implications
To improve people’s access to abortion in the United States, particularly for those with low incomes, policymakers can make policy changes to improve the availability and affordability of telemedicine for medication abortion. They can also make policy changes to improve Medicaid and private insurance coverage for clinic-based abortion.
The Food and Drug Administration regulates the abortion medication mifepristone by a Risk Evaluation and Mitigation Strategy (REMS). This regulation requires that providers must register as certified prescribers and that mifepristone be dispensed directly from a healthcare facility, rather than a retail pharmacy. Despite a growing body of evidence demonstrating that the existing restrictions are medically unnecessary and overly burdensome, the REMS remains.
Removing the REMS classification would increase delivery of medication abortion. In the 31 states that do not ban the provision of abortion by telemedicine, providers could implement flexible service delivery models. Providers could conduct the pre-abortion appointment via telemedicine, and partner with mail-order pharmacies to ship the medications directly to the patient or allow for pick-up at a retail pharmacy. This would allow patients to reduce their trips to the clinic, especially in states with laws requiring multiple trips for pre-abortion ultrasounds or state-mandated counseling. Removing the REMS and making the medications available by mail or pharmacy pick-up would mean fewer trips to the clinic and alleviate some of the burdens such as paying for transportation, childcare, or taking time off of work.
In addition to removing the REMS, Congress could expand affordable abortion access by passing the Equal Access to Abortion Coverage in Health Insurance, or EACH Woman Act. This legislation would repeal the Hyde Amendment and ensure coverage for abortion through all government-sponsored health insurance plans. It would also prohibit politicians from interfering with private health insurance plans that offer coverage for abortion. This would substantially expand insurance coverage for abortion care and would increase the ability of more people, particularly people with low incomes, to obtain an abortion from a medical provider.
Evidence suggests that self-managed abortion will continue, especially as new abortion restrictions are enacted, such as Texas’ recent law prohibiting abortions at around six weeks’ gestation. For people living in the 19 states that prohibit the provision of abortion by telemedicine, self-managed abortion options are especially important.
However, potential legal risks exist for people who self-manage their abortion. Arizona, Oklahoma, Nevada, South Carolina and Delaware have all passed laws criminalizing self-managed abortion, and people in these states could be prosecuted. Moreover, people with few economic resources or those who are members of groups historically criminalized in the U.S. may be at even greater risk of prosecution. Policymakers could eliminate these risks by repealing laws that criminalize self-managed abortion.
Reference
Johnson, D.M., Madera, M., Gomperts, R. & Aiken, A.R.A., The economic context of pursuing online medication abortion in the United States. (2021). SSM – Qualitative Research in Health. https://doi.org/10.1016/j.ssmqr.2021.100003.
Suggested Citation
Johnson, D.M., Madera, M., Gomperts, R. & Aiken, A.R.A. (2021). What motivates people in the United States to seek medication abortion pills outside of the clinic setting? PRC Research Brief 6(11). DOI: 10.15781/xm1d-t214.
About the Authors
Dana M. Johnson, danajohnson@utexas.edu is a PhD candidate in public policy and demography and an NICHD predoctoral trainee in the Population Research Center at The University of Texas.
Melissa Madera is a senior project manager and research fellow for Project SANA (The Self-Managed Abortion Needs Assessment Project).
Rebecca Gomperts is the founder and director of Women on Waves, Women on Web and Aid Access.
Abigail Aiken is an associate professor in the Lyndon B. Johnson School of Public Affairs and a PRC faculty scholar at The University of Texas at Austin.
Acknowledgements
This study was funded by the Society of Family Planning (SFP), Grant # SFPRF12-MA1 and received infrastructure support from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), Grant # P2CHD042849). Neither source of funding had any involvement in the design and conduct of the study; the collection, management, analysis, and interpretation of the data; the preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
About Council on Contemporary Families
The Council on Contemporary Families is a non-profit, non-partisan organization dedicated to providing the press and public with the latest research and best-practice findings about American families. CCF seeks to enhance the national understanding of how and why families are changing, what needs and challenges they face, and how these needs can best be met.