

Sociologists studying emotion have opened up the inner, private feelings of anger, fear, shame, and love to reveal the far-reaching effects of social forces on our most personal experiences. This subfield has given us new words to make sense of shared experiences: emotional labor in our professional lives, collective effervescence at sporting events and concerts, emotional capital as a resource linked to gender, race, and class, and the relevance of power in shaping positive and negative emotions.
Despite these advances, scholars studying emotion still struggle to capture emotion directly. In the lab, we can elicit certain emotions, but by removing context, we remove much of what shapes real-life experiences. In surveys and interviews, we can ask about emotions retrospectively, but rarely in the moment and in situ.
One way to try to capture emotions as they unfold in all of their messy glory is through audio diaries (Theodosius 2008). Our team set out to use audio diaries as a way to understand the emotions of hospital nurses—workers on the front lines of healthcare. We asked nurses to make a minimum of one recording after each of 6 consecutive shifts. Some made short 10-minute recordings. Some talked for hours in the midst of beeping hospital machines and in break rooms, while walking to their cars, driving home, and as they unplugged after a long day. With the recorders out in the world, we couldn’t control what they discussed. We couldn’t follow-up with probing questions or ask them to move to a quieter location to minimize background noise.
But what this lack of control gave us was a trove of emotions and reflections, experienced and processed while recording. One fruitful way to try to distill these data, we found, was through visuals. We created wavelength visualizations in order to augment our interpretation of diary transcripts. Pairing the two reintroduces some of the ‘texture’ of spoken word often lost in the transcription process (Smart 2009:296). The following is from our new article in the journal, Qualitative Research (Cottingham and Erickson Forthcoming).
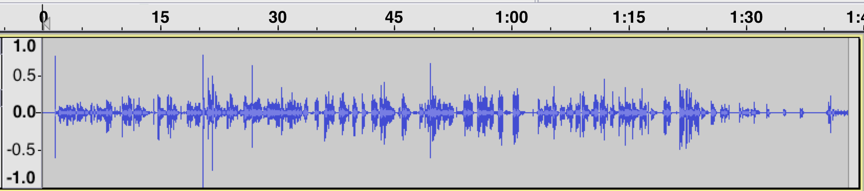
In this first segment, Tamara (all participant names are pseudonyms) describes a memorable situation in which a patient’s visitor assumed that Tamara was a lower-level nursing aid rather than a registered nurse (the full event is discussed in greater detail in Cottingham, Johnson, and Erickson 2018). This caused her to feel “ticked” (angry), which is the word she uses after a quick, high-pitched laugh that peaks the wavelength just after the 30-s mark (Figure 1). The wavelength peak just after the 1:15 mark is as she says the word ‘why’ with notable agitation in ‘I’m not sure why. Maybe cuz I’m Black. I don’t know.’

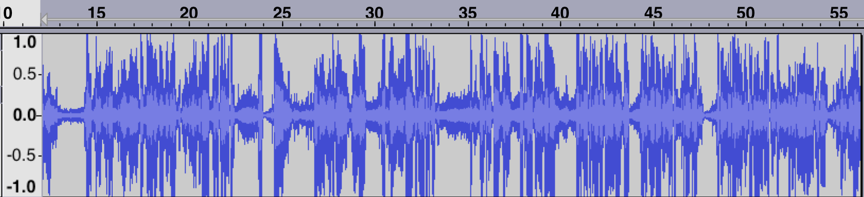
We can compare Figure 1 that visualizes Tamara’s feelings of anger with the visualization of emotion in Figure 2. “Draining” is the description Tamara gives at the beginning of this second segment. The peak just after the 15-second mark is from a breathy laugh as she describes her sister “who has MS is sitting on the bedside commode” when she gets home from work. After the 45-second mark, she has a similar breathy laugh but in conjunction with the word ‘compassionate’ as she says ‘I’m trying to be as empathetic and compassionate as I want to be, but I know I’m really not. So I feel kinda crappy, guilty maybe about that.’ Just before the 1:30 mark she draws out the words ‘draining’ and ‘frustrating’ before finishing: ‘because you leave it and you come home to it…you know…yeah.’ We can see that the segment ends with longer pauses, muted remarks, and sighs, suggesting low energy and representing the drained feelings she expresses, particularly in comparison to the lively energy seen in the first segment when she discusses feeling angry.
A second example comes from Leah, recorded while driving to work. Here she is angry (“pissed off”) because she has to work on a day that she was not originally scheduled to work. This segment is visualized in the waveform shown in Figure 3.
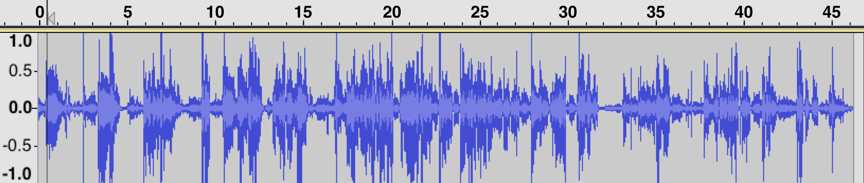
In contrast to her discussion of being pissed off and working to ‘retain enough righteous indignation’ to confront her boss later (in figure 3), we see a different wavelength visualization in her second segment (figure 4). In that segment, she describes her lack of enthusiasm for continuing the shift. She reflects on this lack of desire (‘I don’t want to stay’) by stepping outside her own feelings and contrasting them with the dire circumstances of her young patient. This reflexivity leads her to conclude that she has reached the limits of her ability to be compassionate.
To be sure, waveform visualizations are only meaningful in tandem with what our nurses say. And they do not provide definitive proof of certain emotions over others. They can’t fully identify the sighs, deep inhales, uses of sarcasm, or other subtle features of spoken diary entries. They do, however, offer some insight into how speed, pitch, and pauses correspond to different emotional expressions and, arguably, levels of emotional energy (Collins 2004) that vary across time and interactions.
While there is little that can serve as a substitute for hearing the recordings directly, the need to protect participants’ confidentiality compels us to turn to other means to convey the nuances of these verbalizations. Visualization of wavelengths, in combination with transcripts, can lend themselves to further qualitative interpretation of these subtleties, conveying the dynamics of a segment to others who do not have direct access to the recordings themselves.
Check out the full, open-access article on this topic here and more on the experiences of nurses here.
Marci Cottingham is assistant professor of sociology at the University of Amsterdam. She researches emotion and inequality broadly and their connection to healthcare and biomedical risk. She is a 2019-2020 visiting fellow at the HWK Institute for Advanced Study. More on her research can be found here: www.uva.nl/profile/m.d.cottingham
References:
Collins, Randall. 2004. Interaction Ritual Chains. Princeton, New Jersey: Princeton University Press.
Cottingham, Marci D. and Rebecca J. Erickson. Forthcoming. “Capturing Emotion with Audio Diaries.” Qualitative Research. https://doi.org/10.1177/1468794119885037
Cottingham, Marci D., Austin H. Johnson, and Rebecca J. Erickson. 2018. “‘I Can Never Be Too Comfortable’: Race, Gender, and Emotion at the Hospital Bedside.” Qualitative Health Research 28(1):145–158. https://doi.org/10.1177/1049732317737980
Smart, Carol. 2009. “Shifting Horizons: Reflections on Qualitative Methods.” Feminist Theory 10(3):295–308.
Theodosius,
Catherine. 2008. Emotional Labour in Health Care: The Unmanaged Heart of
Nursing. NY: Routledge.
[
Comments 69
Maryann — November 29, 2019
What nice research! Thanks for sharing! It was very interesting to read! And the visualization is great!
math homework — December 10, 2019
It is not a secret that not everyone can easily solve different math problems easily. But you can always get some assistance from the expert services that can complete your math homework.
https://grademiners.com — December 17, 2019
If you do not know how to write the proper multiple questions for your project, you can visit this link https://grademiners.com to get instant help from the expert services.
ewriters.pro — December 17, 2019
Visit the website of the expert online writing and editing services https://ewriters.pro/ to get the ability to ask the best online writers to write your professional academic paper.
ewriters.pro — December 17, 2019
Visit the website of the expert online writing and editing services ewriters.pro to get the ability to ask the best online writers to write your professional academic paper.
Sameb — January 22, 2020
Nova TV is a brand video streaming app that provides movies and TV shows.
avinash — February 5, 2020
Codm gfx is the best tool for hack pubg and other game have a fun!
avinash — February 5, 2020
tubemate 3.2.14 Best app for download youtube video free.
coca — February 13, 2020
I have read and read a lot of your posts, great, your article has a good and very useful content, thank you for sharing.
vex 3
writing online — February 21, 2020
very important article! Thanks. If you want to know how to express your emotions through writing feel free to visit htts://1ws.com
Alicia — February 21, 2020
very important article! Thanks. If you want to know how to express your emotions through writing feel free to visit writing online
avinash — February 26, 2020
Create and fun with byte
download now make vine videos and short videos
sonam — February 26, 2020
Create and fun with byte app
download now make vine videos and short videos
avinash — February 26, 2020
Create and fun with byte vine 2
download now make vine videos and short videos
Mosedince — February 27, 2020
I would suggest you visit this websitehttps://grandwriters.net/buy-coursework-online. I was looking for some help.
justlearn — March 4, 2020
Amazing to read about this delicious recipe! You always choose a mouth watering recipes like this hot chocolate with white peppermint. I love chocolate recipes thats'why I choose your site to read about it and now I've check more at https://grandwriters.net/assignment-editing-service which I'm able to manage my college thesis task.
Suman — March 5, 2020
I really appreciate this piece of content. Also, see more amazing content like this Easter Instagram Captions
ONE PIECE — July 11, 2020
ONE PIECE TREASURE CRUISE Apk Mod https://apkmodmenu.com/one-piece-treasure-cruise-apk-mod/
Ashley Ridley — August 13, 2020
Studying of emotion is a very interesting thing for me. Actually I want to be a Sociologists but due to my family pressure, I'm a developer now :D This is a funny thing but its true. In this time of the pandemic, emotions can be disturbed due to lock down and everybody is at home. You to chill your mind you should do some mind-blowing. I have an idea and this is the playing of smartphone games and doing home exercises. You can get best free exercise apps for android and enjoy it.
kjwoij — October 30, 2020
How to get a carsforcancer to get some help at the time when i need to visit a doctor for my therapies
Jenny — December 4, 2020
Nice Share!!
Thanks for sharing this useful information and it's worth taking online writing help if you get stuck with any of your assignments or project.
Jenny — December 4, 2020
Nice Share!!
Thanks for sharing this useful information and it's worth taking online writing help from here https://www.cheapestessay.com/ if you get stuck with any of your assignments or project.
Kries — January 26, 2021
Thx my friend!
Anonymous — January 28, 2021
In contrast to her discussion of being pissed off and working to ‘retain enough righteous indignation’ to confront her boss later (in figure 3), we see a different wavelength visualization in her second segment . https://hashalot.io/blog/kalkulyatory-majninga-raschet-pribylnosti-i-okupaemosti-majninga-na-asik-ah-i-videokartah/
Anonymous — January 28, 2021
She reflects on this lack of desire (‘I don’t want to stay’) by stepping outside her own feelings and contrasting them with the dire circumstances of her young patient. This reflexivity leads her to conclude that she has reached the limits of her ability to be compassionate. https://cryptograph.life/kripto-slovar/darknet-darknet-chto-eto-kak-tuda-popast-populyarnye-sayty
alex012 — May 24, 2021
DigitalAkki is best Digital Marketing Agency in Salt Lake City Providing complete Digital Marketing Service in Salt Lake City. If you are looking for Best Digital Marketing Agency in Salt Lake City, No doubt DigitalAkki is best option for you.
Read More
The 5 Best Spy Apps for iOS and Android — June 2, 2021
The 5 Best Spy Apps for iOS and Android in 2021 which can help you to hack enyone you need. I use these apps for a long time and i definitely recommend them for all who want to defend their phone or to check their friends.
Alex012 — June 4, 2021
If you want to learn Digital Marketing and searching for Digital Marketing Course in Chandigarh, you are in the right place. In today’s time, digital marketing is a trendy medium to scale and growth for your career. In this digital marketing course, we give you complete practical training, which provides you with an understanding of working with companies.
Digital Marketing Training,Online Marketing Course
sam012 — June 7, 2021
The Bespoke Group of Entrepreneurs (Bespoke-G-Ent) is a community of like-minded people that interact over startups, networking and trends. Our products are there to serve the needs that an every day entrepreneur may incur. Be it networking, style, productivity or health. We also have an eco-friendly selection.
Bespoke community
sfgcqh012 — June 18, 2021
Locksmith in 77433 – Economical and fast Locksmith professional Service in Cypress,
If you are looking for the best Locksmith in Cypress 77433, Magnet Locksmith is a very good option for you. We Offer excellent and Fast 24/7 locksmith Alternatives Anyplace in Cypress, Texas Region such as Lock Repair, Lockout service, Lock rekey, Office/home/car cupboard locks installation, fixing auto ignition, and all sorts of commercial, non-commercial and automotive locksmith specialist services, modifying the mix of lock, opening the doors, key substitution.
locksmith 77095
Locksmith in 77433
Samuel Wellington — June 25, 2021
Oh great!
https://www.google.com.
Tiffany Walls — June 25, 2021
wow!
google
Alex00 — July 14, 2021
MyInterityCab is your perfect travel partner if you need to hire a car. Our cab rental services range from outstation cabs to airport taxis. Call us to avail affordable one way and round trip offers. Our team is available 24 hours a day before, during and after the car rental takes place, just make your rental experience as smooth as possible.
one way cab
williamwo — August 3, 2021
All I need to unwind a bit is some legitimate flirting. Is this too much to ask? It's nice to know that there are at least review sites that can assist me in my personal life. Similar to Here https://datingadvisor.ca/best-free-online-dating-sites-in-british-columbia-province/ I signed up for a senior dating site.
ghanshyam — November 3, 2021
Are you not getting a job and you are talking here in search of a job, so now you do not need to worry because now you can get a job at the press of a button,
Register now on IndisJob and get the job you want.
Jobs Related Blog
kadın spor ayakkabı — November 9, 2021
kadın spor ayakkabı
kadın topuklu ayakkabı — November 9, 2021
kadın topuklu ayakkabı
retro bowl — January 7, 2022
It is useful information, I have researched it and saved it, will be interested in the next sharing
Steven Johnson — January 20, 2022
Nice thread! Thanks!
John william — January 29, 2022
Technologistan is the popoular and most trustworthy resource for technology, telecom, business and auto news in Pakistan
samsung galaxy A32 price in pakistan
sunny hall — May 4, 2022
This is an excellent blog post. We found the documentation on your site to be quite helpful. The 2 games gartic phone and ovo game that I will introduce today are some of the hottest games today. Let's play and enjoy it
candy — July 1, 2022
You're giving away a fantastic resource, and you're doing so for free. I enjoy reading blogs that recognize the importance of providing high-quality resources for free mapquest driving directions.
Gure — August 23, 2022
But this lack of control made us feel and think about a lot of different things while we were recording. We found that making visuals was a good way to try to make sense of these data. We made visualizations of wavelengths to help us understand diary transcripts better. By putting them together, some of the "texture" of spoken words that is often lost during transcription is brought back (Smart 2009:296). This is from our new article in the journal Qualitative Research (Cottingham and Erickson Forthcoming). backrooms game
anibar.net — November 8, 2022
Your article was great and helpful
The sources from which you have collected information are very reliable and representative.
Thank you very much for this great content
Please also visit my site.
حمل بار به ایلام
حمل بار به سبزوار — November 13, 2022
I really like your content
And I enjoyed your website very much.
I hope you will always be successful
aloobar — November 13, 2022
I really like your content
And I enjoyed your website very much.
حمل بار به سبزوار
John Smith — November 30, 2022
I pretty much love everything about this–nice job!
towingkey
Thelaptops guide — May 31, 2023
Wow, this blog post completely blew my mind! The way you explained the concept was so clear and concise. I can't wait to share this with my friends and colleagues. Keep up the amazing work!"
Also visit this awesome blog - Legenda para foto sozinha
Click here — May 31, 2023
Great
Bimaspin — September 12, 2023
Bimaspin terkenal akan kemudahannya dalam mengakses situs dan kelancaran dalam bertransaksi.
leather motorcycle jacket brown — October 3, 2023
Buy now this jaceket
ساندویچ پانل — October 14, 2023
asia sandwich panel
درب سردخانه
Recycling company in UAE — August 10, 2024
Fascinating insights on visualizing emotions! It really makes you think about how we express feelings
Gamma iptv — March 2, 2025
Gamma IPTV Discover the Best IPTV Gamma Provider Gamma iptv
iptv gamma — March 2, 2025
Gamma IPTV Discover the Best Provider Gamma iptv
iptv gammas — March 2, 2025
Gamma Discover the Best IPTV Gamma Provider
Gamma iptv iptv Gamma
iptv subs — March 2, 2025
Iptv Gamma Discover
Gamma iptv iptv Gamma
abo iptv — March 2, 2025
ABO IPTV Discover the Best IPTV abonnement Provider Abo iptv
iptv abonnement — March 2, 2025
ABO IPTV Discover the Best IPTV abonnement Provider Abo iptv fr
abo iptv — March 2, 2025
ABO IPTV the Best IPTV abonnement Provider IPTV Abo
abo iptv — March 2, 2025
ABO IPTV Provider IPTV Abo
france tv — March 2, 2025
ABO IPTV Discover the Best IPTV abonnement Provider
Abo iptv
France iptv
Ali Raza — April 5, 2025
Auto locksmith course offers specialized training for those looking to master automotive lock and key services. Learn how to handle lockouts, key programming, and ignition repairs with expert instruction and hands-on practice. Whether you're looking to start a new career or expand your skill set, this course provides the knowledge you need. Enroll today in the auto locksmith course to unlock exciting opportunities in the automotive security field!
Masoomen Quran Center — May 26, 2025
very nice keep sharing such a great content with us and Masoomeen Quran Center is an International Quran Academy for Shia Muslims We provide Online Shia Quran Classes Our aim is to educate the youth of the Shia Muslims for making their better future. We work to spread the Quran education across the globe.
harivanshtours — July 8, 2026
thank you so much sharing your knowledge
tempo traveller rental in jaipur
maharanacab — July 8, 2026
very awesome site
Car Rental Service In Jaipur
maharanacabdelhi — July 8, 2026
very useful site
Tempo Traveller Rental in Delhi
agrataxiholidays — July 8, 2026
Lots of information in it thanks for sharing.
Taxi Services In Agra
hielitequartz — July 8, 2026
Great article
Quartz slab Supplier and Manufacturer in India