
Opponents of abortion have long targeted the “demand side” of abortion by passing legislation aimed at dissuading patients from going through with an abortion. Examples of this type of restriction include parental consent/notification laws, waiting periods, and mandatory counseling. Research shows that targeting patients has had little impact on national abortion rates; they’ve been declining, but several factors are likely contributing to the decrease, including increased accessibility to contraceptives.
New approaches to restricting abortion have focused on the “supply side” of the abortion equation — that is, targeting the doctors and clinics that provide abortions. These regulations often require certain staffing and equipment requirements, resulting in clinics being shut down (often due to the expense of implementing the regulations). Reduced access to clinics often means that women have to travel further for an abortion — increasing costs (the procedure itself, travel, and accommodations), especially when a patient has to navigate waiting periods and counseling requirements.
Mississippi’s sole abortion clinic, for example, the focus of abortion opponents for many years, faced closure recently because of a law that changed licensing procedures. The law now requires all doctors performing abortions to have admitting privileges at local hospitals (difficult for the out-of-state doctors to acquire). The clinic was granted an extension to meet the requirements, though the law was allowed to stand.
So, does targeting the supply side of abortion work to reduce the procedure?
A recent article in the New England Journal of Medicine did a natural experiment to answer this question. In 2004, Texas passed two new restrictions on abortion, one on each side. The “demand side” legislation required that women receive information about risks at least 24 hours before an abortion can be performed. The “supply side” legislation required that abortions after 16 weeks of gestation be performed in a hospital or an ambulatory surgical center instead of a clinic. At the time the law was passed, none of Texas’ non-hospital based clinics met the legal requirements, and very few abortions were performed in hospitals.
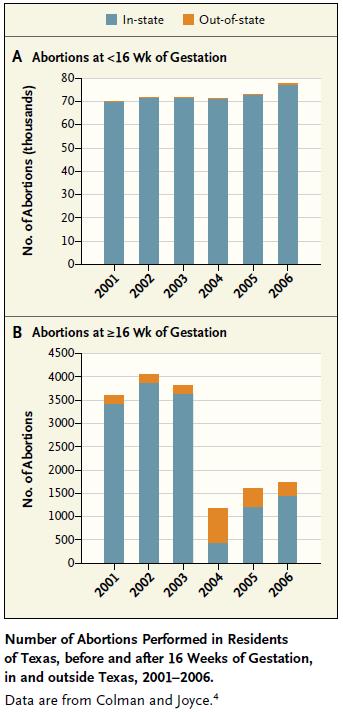
If the “demand side” legislation had an effect, the number of abortions would decrease at all levels of gestation. As Chart A illustrates, there was no change whatsoever in the number of abortions performed before 16 weeks — indicating that the demand side legislation had almost no impact.
If the supply-side legislation had an effect, the number of abortions provided after 16 weeks should have dropped. In fact, Chart B shows that the number of later abortions performed dropped 88% after the legislation was implemented.
So, targeting the supply side reduced the number of abortions performed in Texas, but did the women carry their baby to term?
No. Some of these women left the state to receive an abortion; in fact, the number of who received an out-of-state abortion more than quadrupled from 2003 to 2004. Accordingly, the average distance women had to travel to receive an abortion after 16 weeks increased from 33 miles in 2003 to 252 miles in 2004.
As has been noted on this site before, nations that have highly restrictive abortion laws do not have lower abortion rates; in fact, in those countries where abortion is illegal, many of those abortions are unsafe, resulting in high numbers of maternal deaths. Although targeting the supply-side of abortion might be appealing, it will probably not reduce the abortion rate nationwide. Instead, it likely places onerous restrictions on women with fewer resources, since they will be less able to meet the increased costs that result from having to travel for abortions.
Thanks to Jenna for the submission!
————————
Amanda M. Jungels is a PhD Candidate in the Department of Sociology at Georgia State University, focusing on sexuality, gender, and cognitive sociology. Her dissertation focuses on disclosures of private information at in-home sex toy parties. She is the current recipient of the Jacqueline Boles Teaching Fellowship, given to outstanding graduate student instructors.
Comments 23
Stockholm — July 30, 2012
You mean there is only ONE abortion facility in the WHOLE state of Mississipi ? A state bigger than PORTUGAL ?
Geez, in France we have at least 2-3 per department (http://en.wikipedia.org/wiki/Departments_of_France), and there's 96 of these...
I didn't think the situation could be that disastrous in some US states.
Sam Borchard — July 30, 2012
Just a question: you say that the decrease in abortions after 16 months didn't lead to more women carrying pregnancies to term, but the increase in out-of-state abortions still brings >16wks abortions to just about 50% of what it was before. With no increase in <16wks abortions it seems like there must have been an increase in pregnancies carried to term (or many fewer pregnancies to start with). Am I missing something?
kdlmn — July 30, 2012
The same can be seen in Ireland --> travel to the UK for the abortion rather than decrease in abortions.
TARGETING THE “SUPPLY SIDE” OF ABORTION « Welcome to the Doctor's Office — July 30, 2012
[...] from SocImages [...]
» Cooch Watch Roundup! — July 31, 2012
[...] is also a great piece up on Sociological Images looking at how legislation that targets the “supply side” of abortion effects the women who need access: “Some of these women left the state [...]
Concerned for the Future — January 5, 2013
Personally, I am against abortion, but not against using some form of contraceptive to prevent pregnancy. I believe if people make the choice to have sex in the first place, they MUST be prepared to live with the consequences as well. Some might argue that people shouldn't have to suffer the consequences, that they should do whatever they wish with no fear of repercussions. But, that isn't how the world works. Everything has an effect. If people decide to make the choice, they must live with the results. I am completely against abortion, because though the fetus is not yet creating memories or contributing to society, it is alive. If anything not contributing to society in some way has no right to live, what would happen to our children and our elderly? They do not always directly contribute, in fact, they are generally a drain of resources. But yet the dependent population is the same to society as an unborn fetus is. If it has a heartbeat, it is alive, and a life should not be taken because its caretakers are too afraid or embarrassed to care for it. That is nothing more than cowardice, like Dr. Frankenstein hiding from his creation. Take responsibility for your actions, don't hide it. To quote the immortal words of the beloved Dr. Seuss:"A life is a life, no matter how small." If we take life so wantonly with abortions, how will this casual view of the value of human life spread? If it does, then we have reason to fear for the future of this world...