
With this coming Tuesday marking the 40th anniversary of Roe v. Wade, I’m inspired to post this month’s column early.
I encourage readers to check out the work of ANSIRH (Advancing New Standards in Reproductive Health), a UCSF research program “dedicated to ensuring that reproductive health care and policy are grounded in evidence.” So, rather than cover the breadth of political and social dynamics related to abortion policies, I’m focusing on one specific new study which has important implications for protecting women’s health:
A newly published landmark study by ANSIRH demonstrates that trained nurse practitioners, certified nurse midwives, and physician assistants match physicians in the safety of aspiration abortions they provide. We hope that these results will give policymakers the evidence they need to move beyond physician-only restrictions in order to enable more women to have their reproductive health care needs met in their local communities by health care providers they know and trust.
The results of this study are significant because PAs, NPs and CNMs have been shown to be important and accessible health care providers for rural and low-income women. ANSIRH’s new findings support policies which would reduce health care disparities and increase continuity of care because a larger group of health care providers would be able to offer early abortion care. For more on this topic, read the latest post by Tracy Weitz, Director of ANSIRH. This research should inform health policy across the U.S.
For more on the realities of abortion in the U.S., watch Abortion in the United States, a short video from the Guttmacher Institute.
 Rachel Cheetham Moro used to write a lot about the bollocks of breast cancer on her blog,
Rachel Cheetham Moro used to write a lot about the bollocks of breast cancer on her blog,  *The 2012 edition includes a new Introduction about the Komen for the Cure/Planned Parenthood controversy and a color insert of images of, and reactions to, the pinking of breast cancer. For more information please visit Gayle Sulik’s website at
*The 2012 edition includes a new Introduction about the Komen for the Cure/Planned Parenthood controversy and a color insert of images of, and reactions to, the pinking of breast cancer. For more information please visit Gayle Sulik’s website at 
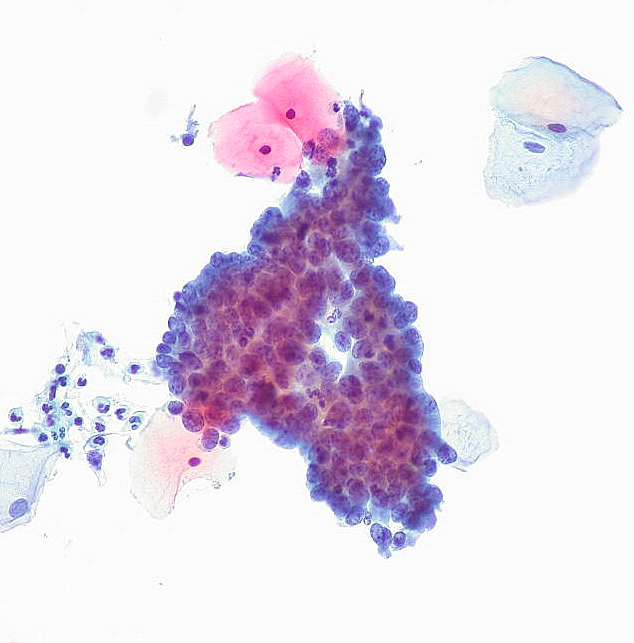
 In light of the new Pap smear guidelines, I hope that U.S. girls and women who get less frequent Pap tests will more frequently ask their healthcare practitioners to educate them about
In light of the new Pap smear guidelines, I hope that U.S. girls and women who get less frequent Pap tests will more frequently ask their healthcare practitioners to educate them about 
