I dedicate this month’s column to parents who are in the midst of crises which are well-articulated on the website A Heartbreaking Choice:
Pregnancy does not end happily for everyone. Sadly, some parents receive grim prenatal news that something is seriously or fatally wrong with their loved and wanted unborn baby. They have to make a decision about continuing or ending pregnancy. We realize that all parents make a loving choice, one they feel is better for their baby. Regardless of the fetal anomaly found, the decision to end a pregnancy is always a difficult one.
Although it is estimated that between 80 and 95 percent of parents receiving a severe prenatal diagnosis choose to end the pregnancy, those who face this nightmare often feel alone. There is very little in the way of support programs for them. With this site and the dedication of courageous parents willing to reach out, we hope to create a safe haven of encouragement, validation, hope and healing.
How many of us have thought about all that is involved with therapeutic abortions? Parents in these situations have to navigate a medical system which is under the influence of a legal system which (in my humble opinion) has succumbed to a failure of the separation between church and state. It saddens and infuriates me that these mothers — especially those in their third trimesters — may be denied access to medical options which could best protect their physical and mental health. In this day and age of U.S. abortion policies, should we be grateful that any states allow any options at all? Gratefulness is hard to come by in the face of so much suffering. My prayers and love go out to all parents who face these heartbreaking choices.

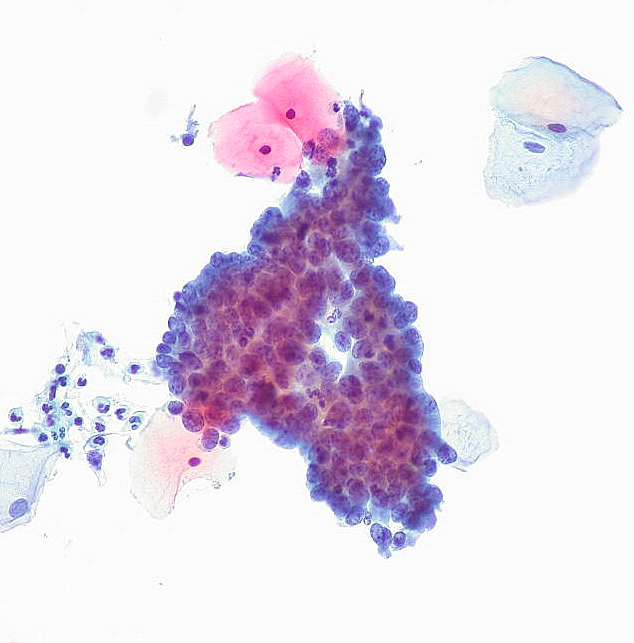
 In light of the new Pap smear guidelines, I hope that U.S. girls and women who get less frequent Pap tests will more frequently ask their healthcare practitioners to educate them about
In light of the new Pap smear guidelines, I hope that U.S. girls and women who get less frequent Pap tests will more frequently ask their healthcare practitioners to educate them about