
A Research Brief Prepared for the University of Texas at Austin Population Research Center
End-of-life planning enhances the quality of later-life caregiving, health, and death. Ideally, informal planning—conversation with loved ones about future care and end-of-life preferences—and formal planning—wills, healthcare proxies, advance care directives, and other legal documents—begins long before the end of life process. Planning is most beneficial when implemented in midlife before people are confronted with debilitating conditions or difficult decisions. Yet only about one-fourth of adults in midlife have advance care directives.
The institution of marriage, particularly heterosexual marriage, involves socially established and legally sustained patterns of norms, roles, values, and behaviors that provide spouses with informal guides to their roles and obligations. Yet norms about husbands and wives taking care of each other “in sickness and in health” may interfere with actually discussing and planning such care prior to serious illness or infirmity. Indeed, studies repeatedly show that heterosexual married couples often do not know each other’s wishes, do not always provide care for each other or receive adequate care from children and extended family, and sometimes even face interference from families.
On the other hand, the institution of marriage is less-established for same-sex couples—marriage only recently became a right and the spouses do not necessarily conform to the marital norms often seen in different-sex couples—which may change the incentives for end-of-life planning. For example, same-sex couples may be less likely to expect end-of-life care from a spouse and therefore be more likely to discuss their expectations for the end of life. In addition, same-sex spouses may worry about encountering discrimination that could lead to family interference and lack of family support and therefore take proactive steps to protect themselves at the end of life. Conversely, they may be wary of going to a lawyer or asking for help from family members because of those same fears of discrimination.
Therefore, formal and informal end-of-life planning unfolds differently for same-sex and different-sex spouses due to different incentives and disincentives that result from the institutional aspects of marriage and higher levels of discrimination against sexual minorities.
The authors conducted in-depth interviews with 90 spouses at midlife in 45 gay, lesbian, and heterosexual marriages. All respondents were Massachusetts residents at the time of the study (2012–2013); Massachusetts was the first U.S. state to legalize same-sex marriage, in 2004. At the time of the interviews, same-sex marriage was not federally protected and was not legal in the majority of U.S. states.
Key Findings
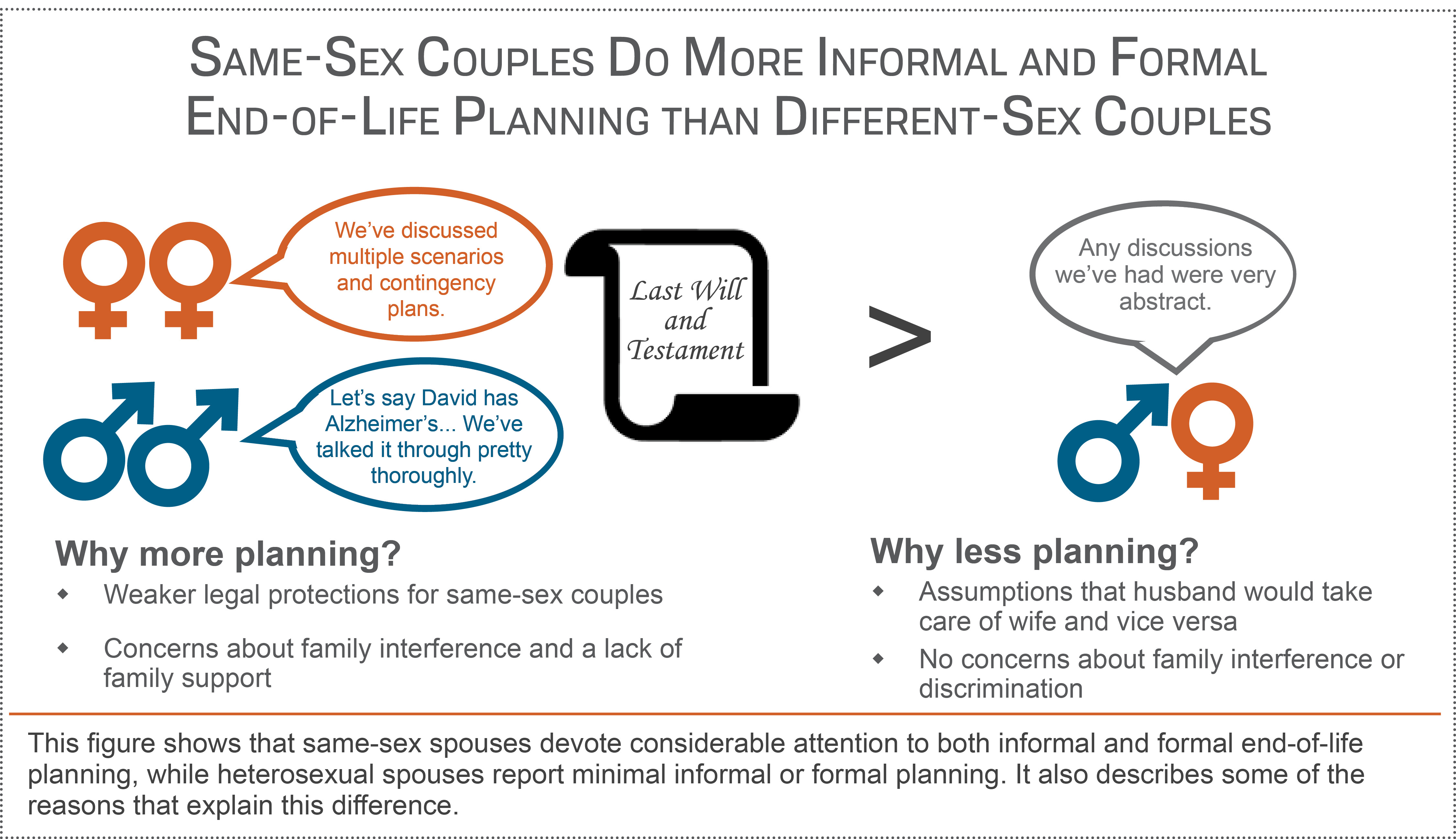
- Informal planning conversations and formal end-of-life plans differ for same-sex and different-sex couples. Same-sex spouses devote considerable attention to both informal and formal end-of-life planning, while heterosexual spouses report minimal informal or formal planning. Two key motivators explain this difference:
- Weaker legal protections for same-sex relationships: Greater engagement in end-of-life planning among gay and lesbian couples has been largely motivated by the weaker legal protections around same-sex relationships, especially prior to legalization of same-sex marriage across the U.S.
- Concerns about family interference and a lack of family support:
- Same-sex couples—especially lesbian couples—expressed concerns about family interference and about a lack of support from extended family at the end of life.
- Heterosexual couples were largely unconcerned about the potential for extended family going against their end-of-life wishes. Therefore, heterosexual couples may be unprepared if they do encounter family interference.
- Couples have different assumptions about what their spouse knows and what family will do at the end of life.
- Heterosexual couples tended to assume that their spouses knew their wishes and that family members (especially adult children) would provide end-of-life care.
- Gay and lesbian couples did not make these same assumptions and instead relied on multiple explicit conversations with spouses and friends about their plans and wishes.
- Same-sex couples often created plans for multiple hypothetical scenarios and worked with lawyers to put legal protections in place.
- Most gay and lesbian couples did not discuss being concerned about lack of family support. Rather, they talked about building strong friendship networks and having explicit conversations with those friends about providing future care.

{kind=link}
Policy Implications
The norms and expectations of heterosexual marriage serve as disincentives for different-sex couples to plan for later-life care and end of life. On the other hand, while gay and lesbian couples may be better prepared for death, their greater planning for end of life may reflect valid concerns about the need for more protection. Recent state initiatives—such as Florida’s proposed bill that would allow hospices to refuse to serve lesbian, gay, bisexual, and transgender adults—indicate that the end of life may actually be a time of heightened discrimination for gay and lesbian couples. Initiatives should aim towards more equality at the end of life. Indeed, policymakers should develop end-of-life planning incentives for all—as well as those not in long-term relationships—which would have the potential to increase well-being for the dying and the bereaved.
Reference
Thomeer, M.B., Donnelly, R., Reczek, C. & Umberson, D. (2017). Planning for Future Care and the End of Life: A Qualitative Analysis of Gay, Lesbian, and Heterosexual Couples. Journal of Health and Social Behavior 58(4):473-487.
Suggested Citation
Thomeer, M.B., Donnelly, R., Reczek, C. & Umberson, D. (2018). Same-sex couples devote more attention to end-of-life plans than heterosexual couples. PRC Research Brief 3(8). DOI: 10.15781/T2RF5KZ8Q.
About the Authors
Mieke Beth Thomeer (mthomeer@uab.edu) is an assistant professor of sociology at the University of Alabama at Birmingham; Rachel Donnelly is a doctoral student in the Department of Sociology and the Population Research Center at The University of Texas at Austin; Corinne Reczek is an associate professor of sociology and women’s, gender, and sexuality studies and a faculty affiliate at the Institute for Population Research at The Ohio State University; and Debra Umberson is a sociology professor and director of the Population Research Center at UT Austin. Thomeer and Reczek are also former Population Research Center NICHD Predoctoral Trainees.
Acknowledgements
This research was supported, in part, by an Investigator in Health Policy Research Award to Debra Umberson from the Robert Wood Johnson Foundation; grant R21AG044585 from the National Institute on Aging (PI: Debra Umberson); grant P2CHD042849 awarded to the Population Research Center at The University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development; and grant T32 HD007081, Training Program in Population Studies, awarded to the Population Research Center at the University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Comments