
Cross-posted at Tim Wise’s website.
It’s one of those stories that can leave even the most jaded and cynical critic of racist thinking scratching their head; the kind that manages to shock even those of us for whom acts of bigotry and intolerance seem all-too-typical, and who have, sadly, come to expect them in a culture such as this.
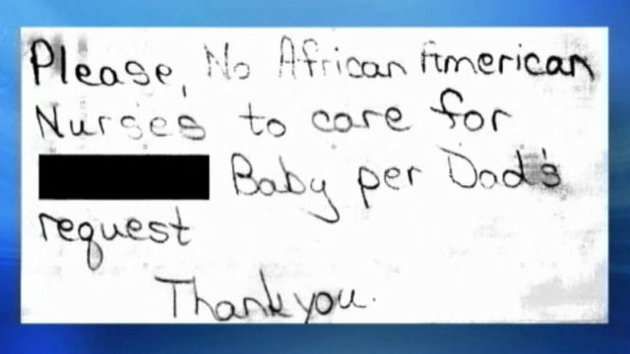
And so it was that in Flint, Michigan recently, a new father — and this is a term he has earned in only the most narrow, biological sense — demanded that when his recently arrived child was sent to the Neonatal Intensive Care Unit of the hospital where she had been born, no African American nurses were to attend to her needs, to care for her, to do what neonatal ICU nurses do, which is to say keep sick babies alive. White hands only for this white, fresh as snow child, whose father, sporting a shiny new swastika tattoo (a Christmas present no doubt from his pathetic skinhead bride) prioritized his own hatreds above and beyond the needs of his precious little girl. That the future does not bode well for her seems hardly worth saying. To be delivered from an ICU into the arms of one as unhinged as this can only, by reasonable people, be seen as a turn for the worse. Incubators and breathing machines might be preferable to having parents such as she has, through no fault of her own, inherited.
But what is worse, perhaps, than the bigotry of this one neo-Nazi — which is at least to be expected and so, can, despite its irrationality in a case such as this, remain somewhat within the realm of the banal — is that the hospital in question, Hurley Medical Center, actually capitulated to his psychotically racist demands, posting a sign on the little girl’s chart instructing the unit to disallow any black nurses from as much as touching this baby.
Presumably, were Tonya Battle, a black Hurley neonatal nurse since 1988 the only nurse within arms reach of the girl as she entered cardiac arrest or as her kidneys began to shut down — both of which have been known to happen to those in a NIC-U — Battle was to scream loudly for a white nurse to come and save the child’s life. Because God forbid a black woman with 25 years experience do the job. And if she dies, well, at least her precious white skin wouldn’t have been sullied by black hands.
Hurley’s acquiescence to this insanity, in contravention of all ethical responsibility, not to mention legal obligations to treat their employees in a non-discriminatory fashion, is going to cost them no doubt, as they are apt to discover once the lawsuit currently brought against their witless administrators plays out. They are going to pay, and pay big, as they should, for their enabling of overt white supremacy. But that is hardly the most important part of this story. Just as it was not the most important part of the story back in 2000 when a heart specialist at St. Thomas Hospital in Nashville did a similar thing, agreeing to the lunatic ravings of another racist white man, who demanded that his wife, who needed open heart surgery to save her life, not be attended to by any black doctor, because he didn’t want a black man to see his wife naked.
More interesting, I think, is what this story (and the earlier one from Nashville) says about racism in America, and not just of the sort evinced by one bottom-feeder, troglodytic fan of Adolf Hitler. For while we are too quick to presume racism to be merely an individual pathology manifested by individually bad people, much like the father in the story from Flint, the fact is, an incident like this illustrates as well as anything can, the way that racism continues to operate as a systemic force in the United States, civil rights laws and all our vaunted post-raciality notwithstanding.
To understand what I mean by this, consider something I am often asked as I travel the country, speaking about racism, or in reply to one or another column or book that I’ve written: namely, it is queried, why don’t I ever talk about black racism, or, just generally, racism against white people? Why, it is wondered, do I focus on racism only when it’s deployed by whites?
There are many things I could say, and do, when asked something like this. But for now, let it suffice to say that this story, from Michigan, involving a white institution as respected as a hospital bending to the whims of a fucking Nazi, is more than enough of a reason for my selective attention. And this is true for multiple reasons.
First, what the story demonstrates is how much more potent white racism is than any potentially parallel version practiced by peoples of color. Simply put, there is no way that any bigoted black person, or Latino, or Asian American, or indigenous person, could possibly have made a similar demand in the reverse direction — that no white nurses attend to their newborn — and expect to have that insistence met with approval and acquiescence. Anyone who thinks a hospital would have agreed to such a thing — to actually deny opportunity to white nurses or doctors, and to limit the care of such a child to same-race caregivers because of the expressed bigotry of a patient — is either so overly medicated or mentally damaged as to make further discussion impossible. In other words, even when a white racist who is likely not of substantial economic means makes a racist demand, his desires can get ratified, and in ways that not even the wealthiest person of color could expect to have happen.*
And this is because — and this is what is especially pertinent to the matter of institutional racism — even if a hospital was willing to go along with the ridiculous and bigoted demands of a hateful person of color, that no whites be allowed to touch their black or brown baby, it would be virtually impossible to fulfill such a request. And why? Simple. Because given the history of unequal opportunity in medical professions, from doctoring to nursing — and also just given the demographic and power dynamics within pretty much any institution you can name — to work around white professionals, even if one wanted to, is almost impossible.
Bottom line: the hospital in this case went along with the demand to exclude blacks from attending to this child because they could. Given the history of discrimination in access to the medical profession, including nursing, and the barriers to professional practice faced by too many people of color, there exists today a more limited number of such professionals from which to draw. As such, excluding them from a particular hospital unit or assignment is hardly a huge burden for the institution in question.
But imagine what would happen if the situation were reversed, and a racist black man had demanded the exclusion of whites from caring for his child. Even if there were a doctor willing to agree to such conditions, it would be virtually impossible for him or her to follow through, because whites — having received the opportunities needed to enter the nursing profession in larger numbers — are hard to work around. “No whites” policies would result in a lot of empty NIC-Us, whereas “No blacks” policies require only a small administrative headache at best, so fewer are such professionals in the first place. And so, given the history of racial inequity, the consequences of which we still experience, white bigotry of the individual type is operationalized and activated if you will, by the institutional injustices that have resulted in the over-represantaion of whites and under-representation of black and brown folks in certain jobs to begin with.
In other words, institutional racism is akin to the gasoline, allowing the otherwise stationary combustion engine of individual racism to function: the former gives the latter life, and the ability to impact others in a meaningful and detrimental way. Without the power to enforce one’s racism, or expect it to be enforced or enforceable by others, that racism is largely sterile. Which is why white racism is simply more worthy of our attention and concern than any other form.
Much the same would be true in other realms of life, beyond medical and hospital settings. Blacks who wish to avoid whites in their neighborhoods will typically find themselves limited to the poorest, most crowded areas of town — places whites long ago abandoned — since finding Caucasian-free zones in more prosperous suburbs can be a tough task. Whites can more or less live wherever we wish. If we are not to be found in a particular census tract you can bet it’s because we’ve chosen to be absent. Such cannot be said for why blacks are often absent from more affluent areas, however. Money or no money, good credit or bad, millions face discriminatory barriers in residential opportunity every year.
Once again, even if people of color despise whites and seek to avoid us, their ability to do so will be directly constrained by the larger opportunity structure that has skewed power and resources in our direction. Whites seeking to avoid blacks and Latinos on the other hand, can do so readily, with the help of mortgage discrimination, redlining, zoning laws and so-called “market forces” pricing many blacks out of the better housing markets (even though we only got into those markets because of government subsidies and preferences, both private and public).
So for those seeking to understand what racism is — and the difference between the merely individual as opposed to institutional forms of it — and why white racism is more potent and problematic than any other potential form, you need look no further than the recent headlines. When institutions can and will collaborate with and directly empower the racism of even the most deranged of bigots, you know that we have yet to arrive at that place of racial ecumenism claimed for us by those who would rather gloss over the ongoing injustices we face, and pretend to have attained, as a people, a perch to which we have no ethical right to lay claim.
————————–
*Please note, I wish to differentiate here between those patients whose desire for same-race/ethnic nurses or doctors is motivated by apparent bigotry, on the one hand, and those whose desire for such a thing might be motivated by such things as linguistic familiarity, on the other. So, for instance, a Spanish-speaking, or for that matter, German or Russian-speaking mother-to-be might request a nurse, or anesthesiologist who speaks their language, for reasons of comfort and communication. Additionally, it is possible that given the history of difficulties in cross-cultural communication between authority figures who are white and patients/clients who are persons of color (which has been studied and documented for years), a black patient might prefer, if possible, to have a black nurse or anesthesiologist to wait on them. Although even these cases are likely rare, they would not be remotely comparable to a blatant bigot demanding same-race care for reasons comparable to the facts in this story, or the 2000 story from Nashville.
————————–
Tim Wise is among the most prominent anti-racist writers and educators in the United States. The author of six books on race in America, he has spoken on over 800 college and high school campuses and to community groups across the nation. His new book, The Culture of Cruelty, will be released in the Fall of 2013.
Comments 114
guest — February 26, 2013
Though this incident is disturbing, I'm sure many will write it off because, hey, it was only one crazy racist guy. But such requests are hardly limited to swastika tattooed patients: See Kimani Paul-emile's study:
Patients' Racial Preferences and the Medical Culture of Accommodation
http://racism.org/index.php?option=com_content&view=article&id=1604:cultureofaccommodation&catid=103&Itemid=269&showall=1&limitstart=
Sei Shonagon — February 26, 2013
I've heard people suggest that the hospital acquiesced to the man's demand because he might have taken the baby out of the hospital and endangered her life. I have a hard time believing that, though. Surely there are hospital guidelines that protect children from the dangerous actions of parents.
Any nurses care to weigh in? I'm curious.
Tusconian — February 26, 2013
I generally like Tim Wise ok, and generally agree with him here, but I think his own experiences have colored his perception of exactly how easy it would be for a nonwhite patient to demand no white nurses care for them. I can not remember ever meeting a white nurse in a hospital or nursing home. Nursing is one of the few careers, much less science-based careers, that nonwhite women are legitimately encouraged to pursue. You'll notice the man in the story never had to make the demand that no black doctors care for his wife, and still made the demand about nurses. In Flint, Michigan? Very likely, black nurses were the majority of nurses, but there were so few black doctors that it didn't even cross his mind to request one, and from what I know, not enough Latino or Asian employees to even ping on his radar. Wise is right, a nonwhite person likely wouldn't be able to make this demand and have it be taken seriously, but it's not for lack of nonwhite nurses in predominantly nonwhite areas.
Granted, this is mostly, if not entirely, based on the fact that every hospital I've been in has been in a predominantly black area of a relatively segregated city with a high level of immigration from non-white countries. But, many, many black people live in such areas, so it seems rather silly for a white man to claim that the request couldn't be made simply due to it being impossible due to white people invading every occupation. Maybe not in Tim Wise's neck of the woods, but I doubt that's terribly representative of the average urban, working class black person's experience. I know this is a nitpick, but since so many other anti-racist white folks take basically everything Wise says as law, I think it does matter when an unrealistic statement like that is made.
mimimur — February 26, 2013
Fantatstic, this is an argument that I have needed for ages, and it can be applied to other human rights issues as well.
John Tantalo — February 26, 2013
What do you mean by "white institution"?
Rishi — February 26, 2013
"I am often asked as I travel the country, speaking about racism, or in reply to one or another column or book that I’ve written: namely, it is queried, why don’t I ever talk about black racism, or, just generally, racism against white people? Why, it is wondered, do I focus on racism only when it’s deployed by whites?"
Because I don't earn any lefty social capital by talking racism against whites, so I just mumble something about there not being enough non-white nurses or something, which anyone who has ever visited a hospital in any metro area in the U.S. knows is total bullshit.
Edited for honesty
Brianna Gamma — February 26, 2013
Patients are allowed to refuse care from a provider for any reason, however stupid and racist. It's very common for men to refuse to be treated by women, or women by men, or blacks by white doctors. In some places you can specify Christian staff. I suspect that if there was an emergency the sign would be disregarded, and that it was mostly for the routine care.
If a black father for some reason made this request, likely it would be honored in the same way-- for non-emergencies, if the staff were availiable. I suspect it would be impossible to insist that only people of East Asian ancestry or Native ancestry tend to your child, but a hsopital will rejigger things so a SPECIFIC nurse tends to a SPECIFIC child if the patient asks (a coworker went to the same hospital for both her deliveries, for example, and when she saw a nurse she liked from before, she specifically asked to have that nurse care for her and they rearranged things to oblige her), so it's not too strange to see them obliging stupid requests.
Of course we need to get rid of the underlying prejudices as best we can.
lia — February 26, 2013
This is a little off-topic, but was the completely ableist sentence needed? "Anyone who thinks a hospital would have agreed to such a thing — to actually deny opportunity to white nurses or doctors, and to limit the care of such a child to same-race caregivers because of the expressed bigotry of a patient — is either so overly medicated or mentally damaged as to make further discussion impossible."
As a radical-minded intersectional socialist who lives with severe medication-resistant psychiatric disabilities, I don't even have words for how wrong it is to correlate mental with racist thinking or acts. It is not okay to make your point with ridiculous ableism such as this, especially when you offer no citations to back up your claim. This is just more faux-left, liberal minded bullshit and I am so tired of it.
Anna — February 26, 2013
It seems to me that the people who have already commented on the post in a critical way are doing so with a heavy heart. This post is both passionate and informative, and Wise is deeply invested in his subject matter. So it sort of pains me to criticise this post, but well, it's just a very weak explanation of what makes white racism systemic. I have to gather my thoughts before I write a post on why, but other commenters have already started to pick apart at the seams. Just the last paragraph alone, which is strangly presented almost as an afterthought, would blow apart Wise's explanation if you delved into it with more precision. Wise is very timid in exploring the reasons people request specific race/ethnic health-care professionals.
*Systemic* social phenomenons, such as white racism (let's say white racism in North America so we don't overstep and make errors), are a key idea of sociology; they drives most, if not all, of sociological theory. If you can't make a case for a phenomenon being systemic, you don't have a case, no matter how worthy your cause is. No matter how heartbreaking the indignities you are fighting against are. Harsh, but true. Emotional appeals, pointing out how unfair and unbalanced something is, these all can serve an important purpose for driving social change, but they are NOT sociological. One must establish what 'systemic' means in the first place, which this post gets partly wrong, and it happens to be an important part to get right.
It's just really, REALLY important to present a cohesive, bullet-proof explanation of what makes white racism a systemic phenomenon, even though you'll have people who disagree with you, including intelligent, well-informed and educated people. Fair enough. If your argument is strong, you can still stand by it, still heavily utilize it to teach a class or participate in a grassroots social movement, or even stand up for yourself or someone who is disenfrachised. But Wise is presenting 1) a SITUATIONAL phenomenon, as in the example of there not being enough black nurses and doctors, which is sociologically problematic simply for being situational, but even more so because, as per the comments, it isn't even true. And that's not even the only example he uses that is situational. And 2) He is mistaking SYSTEMIC for BELIEFS/OPINIONS THAT ARE SHARED BY A SIGNIFICANT AMOUNT OF PEOPLE. That's actually how people justify "reverse" racism and other forms of discrimination.
For example, tons of black people think white people are stupid and think their skin is pig-like and gross, snd would never hire them, would disown their own children for shacking up with a white person, and might beat them to a pulp in a predominantly black-populated environment: that's racism! Statistically, more black people hate white people than vice versa (as in South Africa where the dominant population is black): omigod, black people are even more racist than white people! Tons of poor people absolutely hate rich people's guts, spit in their food, 100% justify stealing from them and doing other material and/or emotional harm to them, and basically wish they were dead: that's oppression! And there are way more poor people in the world who hate rich people than vice versa: oh my god, rich people are even more oppressed than poor people!!
Both examples are sadly very true. But they are NOT examples of racism and oppression. See, in another contexts, I would be open to debating the validity of the gray matter in between racism and non-racism, and the murky waters of what counts as systemic as opposed to what doesn't. There are some decent debates and counter-arguments lurking out there. But Wise is not helping his case if he thinks this post is a strong example of systemic racism.
Eric — February 27, 2013
Lia. Radical blah blah socialist? No one will read that. Well.. I did. Folks think whatever they want. There is no agenda. Just opinions. Go easy.
[links] Link salad’s mind is not for rent | jlake.com — February 27, 2013
[...] Reflections on Racism, Both Individual and Systemic — This story depresses me profoundly. [...]
Guy — February 27, 2013
To be honest your use of foul language damages your message.
susie — February 27, 2013
My brother is white, American-born, and schizophrenic. He has had to ask to speak to an English speaking mental health professional when hospitalized in Miami. So, yes, there is a distinction between racism, and communicating with your doctor in your native language.
TK — February 27, 2013
'Without the power to enforce one’s racism, or expect it to be enforced
or enforceable by others, that racism is largely sterile. Which is why
white racism is simply more worthy of our attention and concern than any
other form.'
Thank you so much for this! I've been looking for a brief, clear way to express just this idea (for this and some other -isms).
Sonya Kiersky — February 27, 2013
Tim, this post is, in my opinion, an example of everything that is wrong in recent discourse on race relations and the exact reason why laypeople think that 'reverse racism against white people' is now a rising issue. If you want some background I am female, non-white, and also work in a hospital. The full trifecta! I feel compelled to list my demographic stats before posting, out of fear that my arguments will be dismissed as "Nazi thoughts" otherwise.
Argument 1): Poorly written, using vague self-justifying phrases such as "in a culture like this...XYZ is wrong" as the core of your argument. Lots of leading language actively disparaging the white couple as 'Nazis', followed by an emotional ("you don't want to support Nazis, do you?") argument as opposed to a logical argument/critical analysis of why this couple might think the way they do.
Argument 2): Facts (that other ethnicities would not be catered to if they wrote a note like this) are not correct. I work in a hospital, and many patients do in fact request doctors/nurses that are of the same gender/race/home language as them. Hispanics, blacks, whites, asians, females, males....people generally prefer others who look and talk as they do, and who understand the cultural context they are coming from in terms of what medications and treatments they consider appropriate. While on different nursing units, I have had Spanish-speaking patients, African-American patients, religious patients, etc. request contact from specific nurses only who were of the same cultural background as them. These are people going through extremely painful patches in their lives emotionally/physically so yes, a large hospital WILL go out of its way to give them familiarity and comfort.
Of course, if you do not think that 'white people' in the US (ie generally British/Scottish/Irish/Germanic descent) have a common and valid culture that is (like all cultures are) distinct and different from other cultures, and if you therefore believe no white person should ever feel a cultural need to be in the company of other white people....you are a strange and misinformed human.
Argument 3): Misunderstanding of what racism means. Maybe we grew up reading different Racism 101 textbooks, but in my book a hospital patient requesting a Spanish-speaking nurse, a white nurse, a male nurse, etc. etc. is a personal preference, and personal preferences are not a problem/should not be disparaged. It is petty and childish to write an entire article making fun of a couples' personal preferences. I have requested female-only staff before when I have been in the hospital, as well as only nurses/doctors of my ethnicity in certain culturally sensitive situations regarding the treatment of family members.
Racism is when an _institution_ or _society itself_ prefers a certain type of person (ie: if the ENITRE HOSPITAL had a 'No African-American nurses' sign, a policy on kinky hair being unprofessional, etc). The solution to racism is not to 'thought-police' people and ensure they have no pride in their own race/background...but to hire a diverse group of people to upper-level positions so that each of their personal preferences cancel out, so to speak, and the OVERALL institution is run neutrally.
ViktorNN — February 28, 2013
2 points:
1) Are any white people reading this post really persuaded or consoled by the argument that incidents of racism perpetrated against them are "constrained by an opportunity structure" that supposedly "skews power and resources" in favor of whites?
I mean, incidents of racism are incidents of racism and if you're the victim, the effects are terrorizing no matter what the skin color. I don't see why white people don't deserve an equal voice at the victim's table when they commit disproportionately fewer hate crimes than other groups, and are disproportionately more likely to be victims of interracial crime.
Take for example this recent case against a white elderly woman.
http://www.dailymail.co.uk/news/article-2229645/Two-male-nurses-caught-camera-sexually-abusing-98-year-old-stroke-victim-paid-55-day-care-of.html#ixzz2C1fKBRSX
To my knowledge the racist subtext which is almost certainly present wasn't even addressed in the case, and yet Wise asks us to consider racist attacks against white as somehow different and lesser.
Any white person who buys this should seriously look into getting a backbone.
2) When Wise talks about white people he repeatedly refers to himself as white, using the pronoun "we." Wise is being dishonest or at least opportunistic here - he is most definitely not white by many definitions. The fact that he glosses over his identity always makes me suspicious of his arguments and makes me wonder what else he might be glossing over.
Zora — March 2, 2013
I once had an elderly man ask me to call the cops so that he could report the theft of his car. He also asked that I request that they not send a "lady cop". I was outraged, but my co-worker considered it since he was so old and could therefore be expected to be sexist like that. Of course, I made no such request and was quite pleased when it was a "lady cop" who happened to arrive.
nope — June 9, 2013
only white people. they are the most racist people on earth.
Jack William — February 22, 2022
Try to sign up for as many affiliate programs as possible, because this way your chances of making a sale increases significantly. https://adelaidetherapy.com/1555-2/
Dean Marsh — September 29, 2025
You may mix and match these in a million different ways to make fun solar smash games, puzzles, or experiments.
elongrimer — December 2, 2025
To my knowledge the racist subtext which is almost certainly present wasn't even addressed in the case, and yet Wise asks us to consider racist attacks against white as somehow different and lesser smashy road free.