An emerging controversy in Canada is a good example of just how difficult it is to be racially-neutral when the context is racially-charged. The country recently redesigned its money. On the back of the $100 dollar bill celebrating medical innovation they sketched an Asian-appearing woman looking into a microscope. In a focus group in Quebec, people complained that the bill reproduced the stereotype that Asians pursue careers in science and medicine. The Vancouver Sun reports:
“Some have concerns that the researcher appears to be Asian,” says a 2009 report commissioned by the bank from The Strategic Counsel… “Some believe that it presents a stereotype of Asians excelling in technology and/or the sciences. Others feel that an Asian should not be the only ethnicity represented on the banknotes. Other ethnicities should also be shown.”
A few even said the yellow-brown colour of the $100 banknote reinforced the perception the woman was Asian, and “racialized” the note.
The Canadian government responded that they had never intended the woman to appear “ethnic” and ordered the image re-sketched so it would be more racially “neutral.” 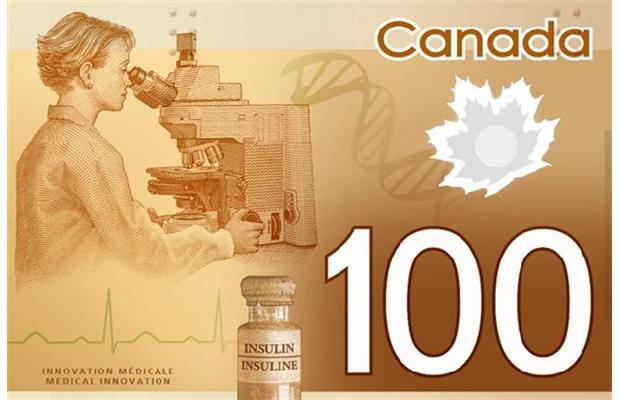
They were then accused of being prejudiced again. Mu-Qing Huang, a Chinese-Canadian interviewed for the story, objected to the deletion of the figure’s Asian features:
If Canada is truly multicultural and thinks that all cultural groups are equal, then any visible minority should be good enough to represent a country, including (someone with) Asian features.
This is a tricky problem. By including racial or ethnic minorities on their bills, Canada risks reproducing a stereotype. Including all “neutral” figures can be seen as exclusionary because neutral looks suspiciously like White people in a country dominated by White people. The third option is to deliberately break stereotypes by putting, say, an Asian woman running the hurdles and a Black woman looking through a microscope, but this can seem overly contrived (as many attempts at diversity do).
The truth is that all of Canada’s options can be read in racially-charged ways. This isn’t because people are unfairly reading into the sketches, it’s because life in Canada is, in fact, racially-charged. When race matters, it matters, all claims to colorblindness aside.
Thanks to Craig G., Tom Megginson, Jesse, Helen, and Alex, an MLIS from McGill, for the submission!
Lisa Wade, PhD is an Associate Professor at Tulane University. She is the author of American Hookup, a book about college sexual culture; a textbook about gender; and a forthcoming introductory text: Terrible Magnificent Sociology. You can follow her on Twitter and Instagram.