
In honor of April being STD Awareness Month, I devote this month’s column to a topic that remains near and dear to my heart (and my cervix): HPV, human papillomavirus. So, it’s a great time to get yourself tested at your local STD testing location, or send an e-card to a loved one who could use a friendly reminder:

 This month might have inspired some of you to consider vaccines that offer some protection against HPV: like Gardasil or Cervarix.* However, don’t get too excited about Gardasil if you happen to be 27 years old (or older) and live in the U.S. Earlier this month, the FDA decided against expanded the vaccine’s label use for ‘older’ women:
This month might have inspired some of you to consider vaccines that offer some protection against HPV: like Gardasil or Cervarix.* However, don’t get too excited about Gardasil if you happen to be 27 years old (or older) and live in the U.S. Earlier this month, the FDA decided against expanded the vaccine’s label use for ‘older’ women:
However, as of Tuesday, ‘older’ Canadian women now have more options than their U.S. counterparts:
So, what’s the deal? According to a Canadian women’s health expert, this is a good decision:
If I’m correct in inferring that Dr. Ferenczy’s use of the phrase “social status” refers to a woman’s sexual partner/sexual relationship status, then are we to assume that U.S. women between the ages of 27 and 45 are in more stable sexual relationships than their Canadian counterparts? I’ve yet to read a study that would support this conclusion.
So, as a U.S. woman who happens to be in this age group, I feel it only right to encourage my peers to ask their doctor about Gardasil, especially if they’re “changing their social status.”
For the boys and men out there, remember that the FDA approved Gardasil in October 2009 for protection against two types of HPV which cause genital warts in males ages 9-26. Then, last December, the FDA approved of GARDASIL for the prevention of anal cancers caused by two different types of HPV in females and males 9-26 years old.
However, once again, there appears to be possible age-discrimination: men over 26 years old, consider whether Gardasil might offer health benefits for you.
*Note to readers: I respect that many will decide that a vaccine is not right/healthy/safe for themselves or for their family members. I highlighted the recent news about Gardasil because I believe that everyone deserves access to vaccine updates. I’ll conclude by quoting myself:
I don’t know if the pro- and anti-vaccine folks will ever see eye to eye, but there’s absolutely nothing to lose and everything to gain by being pro-HPV-education.
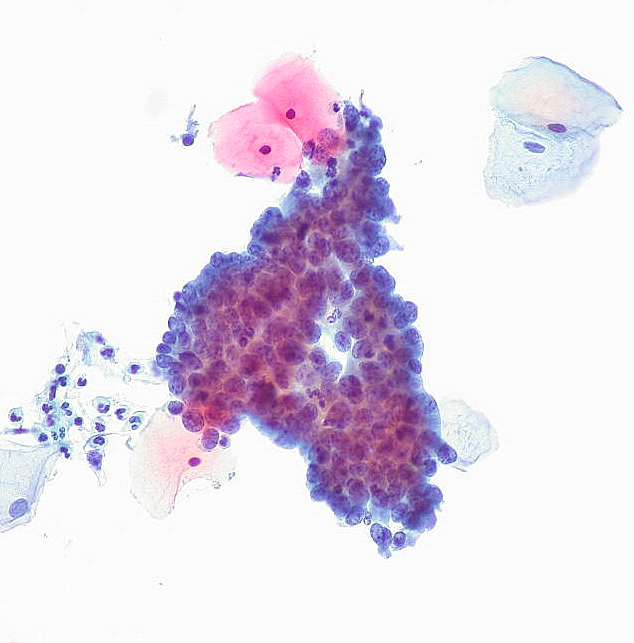
 In light of the new Pap smear guidelines, I hope that U.S. girls and women who get less frequent Pap tests will more frequently ask their healthcare practitioners to educate them about
In light of the new Pap smear guidelines, I hope that U.S. girls and women who get less frequent Pap tests will more frequently ask their healthcare practitioners to educate them about 